
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a E-poster Indonesia care quality: accreditation or payment system
Semelhante a E-poster Indonesia care quality: accreditation or payment system (20)
Último
Último (20)
E-poster Indonesia care quality: accreditation or payment system
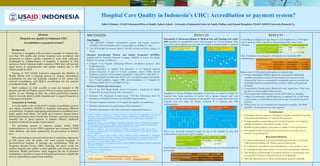
- 1. Hospital Care Quality in Indonesia’s UHC: Accreditation or payment system? Abstract Hospital care quality in Indonesia UHC: Accreditation or payment system? Background Indonesia is struggling with provision of quality of medical care. Less than 30% public and private hospitals were accredited; and investment to achieve quality standard is more than sufficient. Challenged by maldistribution of hospitals, it launched in 2014 ambitious Social National health insurance (SHI) that will provide equal access of comprehensive and quality medical care to 250 million people by 2019. Starting in 2013 USAID Indonesia supported the Ministry of Health (MoH) with a learning process to achieve international accreditation for nine top hospitals, adoption of JCI criteria into national accreditation, and ISQUA accreditation for the national accreditation body - KARS. MoH continues to fully accredit at least one hospital in 500 districts and 50% of Primary care by 2019 as to ensure equal access to quality of care. Starting in 2016, the central government transfers fund to renovate district public hospitals and to support hospitals in achieving accreditation Assessment & Findings A 4 year study is also conducted to examine accreditation process and impact evaluation (HAPIE) in hospitals undergoing different accreditations. Hospitals undergoing international accreditation have better quality than others. The study also monitors changes before SHI implementation and 6 month later. It shows a general worsening situation due to sharp increase of patients without additional hospital investment for quality improvement. For providing options to improve quality within SNHI implementation, we review SNHI regulation and structure of SNHI claim database, and study qualitatively the governance of medical care. SHI credentialing is not materialized due to mandatory agreement of SHI payer with all public and some private hospitals. It dis-incentivizes hospital to undergo any accreditation. With the Diagnosis Related Group (DRG) claiming, the payer could not monitor hospital care quality in most globally used clinical practice indicators. Health governance study suggests the use of payment mechanism to incentivize improved hospital performance despite the need to unbundling hospital claim database. Edhie S Rahmat - USAID Indonesia/Office of Health, Anhari Achadi – University of Indonesia/Center for Family Welfare, and Edward Broughton, USAID ASSIST/University Research Co. METHODS Two Studies: 1. The 2013-2016 Hospital Accreditation process and impact evaluation (HAPIE): Does accreditation have a strong impact on Quality of Care? 2. The 2015 Health Governance Review: Do SHI policies incentivize Quality of Care? Hospital Accreditation Process and Impact Evaluation (HAPIE), implemented by University Research Company (ASSIST) & Center for Family Welfare –University of Indonesia: • Compare 9 top hospitals undergoing different accreditation processes (JCI, KARS and none) • Patient perception of Quality: Exit Interviews of 30 randomly selected patients/care-givers in each of 4 wards (pediatric, surgery, OBG, internal medicine), total 2,167 in all hospitals for period of August 2013 vs July 2014 i, ii • Collecting hospital secondary data (LOS, Care Costs paid by patient and deaths) from 4 wards (pediatric, surgery, OBG, internal medicine) in 9 hospitals for period Jan-March 2014 vs. Jan-March 2015 iii Review of Health Care Governance: • Part of the 2015 Rapid Health System Assessment – conducted by Health Finance & Governance project (Abt Associates) iv • Reviewed >50 documents & interviewed >150 Key Informants from 65 institutions on Health Governance in early JKN implementation • Identified regulatory incentives for Hospital Care Quality (Accreditation) v • Identified opportunities for performance-related payments vi • Identified information system that could track hospital performance vii RESULTS Perceptions of Decreased Quality of Medical Care and Nursing Care under SHI regardless of accreditation status, with exception of C & D hospitals. This shows that most hospitals were not ready for sharply increased number of patients after SHI implementation. Timeliness of Service & Patient perception of how they are treated by Staffs: JCI hospitals have better timeliness of service, but in general hospital staff were perceived to provide worse treatment in all hospitals. This is again shows that most hospitals were not ready for sharply increased # of patients after SHI implementation. There were increased in-patient’s length of stay in all hospitals in early SHI implementation, but shorter in JCI hospitals. Total hospital cost per in-patient case is also increased, and even increased higher in JCI hospital. For additional information please contact: Edhie S Rahmat, USAID Indonesia/Office of Health - erahmat@usaid.gov RESULTS Controlling for diagnostic & age; Patients in JCI hospitals have a 37% higher risk of death (p<0.001); and risk of death increased 49% more in JCI Hospitals. Risk of deaths are also changed in all hospitals at 6 month after SHI implementation. Rapid review of SHI policies and regulations concludes that: 1. Facility credentialing: Public hospitals are automatically credentialed, regardless accreditation status; Private hospitals that were previously contracted by Askes are automatically credentialed; and new providers are credentialed based on meeting human resources, facility, and equipment standards. 2. Comprehensive benefits were offered with some negative lists. There is no priorities to certain public health concerns. 3. The hospital claim reimbursement system (INA-CBG) are bundling coding, no performance related indicators, un-updated cost, over & under compensation to certain clinical interventions and no incentive for good practices. 4. Efforts focus on Cost containment by instituting committees like BPJS and HTA, but decisions lie on other agencies. i. Latief, K., Nandiaty, F., Pawestri, E.A., Wahyuni, S., Rianty, T., Achadi, A. 2015. Presentation in 2015 APACH Conference “Patient satisfaction at the early stage of National Health Insurance (NHI) implementation: A comparative study before and after NHI implementation at nine class A public hospitals in Indonesia “ in Bandung, October 22, 2015. ii. Broughton E, Achadi A, Latief K, Nandiaty F, Nurhaidah, Qomariyah SN, Rianty T, Wahyuni S, Eskaning AP. 2015. Hospital accreditation process impact evaluation: Midline report. Technical Report. Published by the USAID ASSIST Project. Bethesda, MD: University Research Co., LLC (URC). iii.Broughton, E., Anhari, A.. 2015. Recent presentation of HAPIE midline findings to BPJS –Health “What questions can BPJS data answer in the HAPIE Study?” in Jakarta, December 12, 2015. Data was collected from BPJS database. iv. Hatt, L., Altea, C., Chee, G., Ergo, A., Fuad, A., Gigli, S., Hensley, L., Laird, K., Ramchandani, N., Simatupang, R., Tarantino, L., Wright, J., Zuwasti, U. December 2015. Rapid Analytical Review and Assessment of Health System Opportunities and Gaps in Indonesia. Bethesda, MD: Health Finance and Governance Project, Abt Associates Inc. This is available for public access in https://dec.usaid.gov/dec/content/Detail.aspx?ctID=ODVhZjk4NWQtM2YyMi00YjRmLTkxNjktZTcxMjM2NDBm Y2Uy&rID=MzczMDYx v. **See section on Service Delivery of Public and Private Sector” vi. ***See section on Health Financing vii.****See section on HIS -3 -6 2 2 -9 -6 -14 -3 -3 -4 -20 -15 -10 -5 0 5 10 15 20 A B* C D E* F* G* H I All Upper Lower Percentage Graph#1 % Change in Quality of medical Care (p≤0.05) -6 -7 -2 3 -14 -9 -12 -5 -2 -6 -20 -15 -10 -5 0 5 10 15 20 A* B* C D E* F* G* H* I All* Upper Lower Percentage Graph#2. % Change in Doctor’s competence (p≤0.05) -3 -3 2 -2 -9 -6 -13 -8 -5 -5 -20 -15 -10 -5 0 5 10 A B C D E* F* G* H* I* All* Upper Lower Percentage -2 -2 4 4 -8 -1 -8 -4 -1 -2 -20 -15 -10 -5 0 5 10 15 20 A B C* D* E* F G* H I All* Upper Lower Percentage Graph#3. % Change in Quality of Nursing service (p≤0.05) Graph#4. % Change in Nurse/Midwife’s competence (p≤0.05) 4 -2 7 -15 -8 -7 -13 -6 -12 -6 -20 -15 -10 -5 0 5 10 15 20 A B C* D* E* F* G* H* I* All* Upper Lower Percentage -10 -7 -7 -11 -29 -14 -13 -16 -13 -13 -35 -25 -15 -5 5 15 25 A* B* C* D* E* F* G* H* I* All* Upper Lower Percentage Graph#6. % Change in Timeline of Service (p≤0.05) Graph#7. % Change in Staffs’ Treatment (p≤0.05) Conclusions: 1. Accreditation has less impact to Perception of Quality and Patient Outcome at the early implementation of Social Health Insurance. 2. Though mandatory credentialing, there is limited incentive for hospital to undergo accreditation and maintain quality of care. 3. Bundled hospital claiming system limits the ability to show performance. 4. SHI regulations limit the performance based payment and provision of incentive for good practices. Recommendations: 1. To start incentivizing good practices through payments (for e.g. Hospital Value-Based Purchasing, UK Quality outcome framework). 2. To complement accreditation and credentialing to ensure quality of care. 3. To unbundle hospital claim system to show certain performance indicators. 4. Start thinking of global budget to hospitals and link it to performance (for e.g. Inpatient Prospective Payment System in US Medicare). 5. Start with admission rate to observe performance and grow gradually.