
Recomendados
Mais conteúdo relacionado
Semelhante a Obstructive Airway Diseases.pdf
Semelhante a Obstructive Airway Diseases.pdf (20)
Último
Último (20)
Obstructive Airway Diseases.pdf
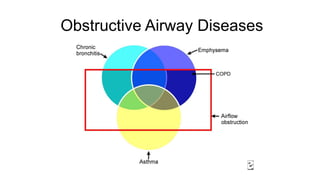
- 2. Obstructive Airway Diseases ● COPD ○ Chronic bronchitis ○ Emphysema ● Asthma ● Bronchiectasis
- 4. COPD Chronic Bronchitis ● Persistent or recurrent excess of secretion in the bronchial tree on most days for at least 3 months in the year, over 2 years ○ Mucous gland hyperplasia ● Risk factors ○ Cigarette smoke ○ Air pollution ○ Dust exposure - cadmium ○ Infection Emphysema ● Characterised by abnormal, permanent enlargement of the airspaces distal to the terminal bronchioles, and destruction of their walls without fibrosis ○ Loss of elastic recoil ○ Airway narrowing ● 3 morphological patterns ○ Centriacinar ○ Panacinar ○ Paraseptal
- 6. COPD Exacerbation - COPD X ● Usually multifactorial ○ Infection - viral, bacterial ○ Medicine non-compliance ○ Iatrogenic ● History ● Exam ● Bloods +/- ABG ● ECG ● PFTs ● CXR Management ● O2 ○ Controlled via Venturi if CO2 retainer ○ Otherwise high dose via face mask ● Nebulizers ● Steroids ● Antibiotics ● Diuretics ● BiPAP
- 8. Asthma ● Hyperreactive airways leading to episodic,reversible bronchoconstriction, owing to increased responsiveness of the tracheobronchial tree to various stimuli ○ Atopic ○ Non-atopic ● Non-specific triggers ○ Exercise ○ Cold air ○ Emotional distress ○ Aspirin/NSAIDs
- 11. Asthma Presentation 1. History a. Precipitating factors b. Previous attacks c. RF - ICU, Comorbidities, Compliance 2. Exam a. Inspection b. Vitals c. Auscultation d. PEF/FEV 3. Investigations a. Bloods/ABG b. CXR? Initial Management ● Position ● O2 ● Salbutamol nebs ● Ipratropium nebs ● Steroid ● IVH - insensible losses
- 12. Status Asthmaticus ABG - Hypoxia, Hypercapnia, Acidosis, Hypokalaemia
- 13. Advanced Management ● IV Magnesium ○ 2g over 20 minutes (up to 6g) ● IM Adrenaline/IV Adrenaline ● IV Salbutamol ○ 3-6ug/kg over 5 minutes ○ Infusion 10ug/min (titrate up to 40-60ug) ○ ECG - arrhythmias ○ Bloods - hypokalaemia, lactic acidosis ● IV Ketamine ○ Pre-induction/Induction
- 14. Mechanical Ventilation ● Increases both morbidity & mortality ● Pre-oxygenation - BiPAP ● Avoid hyperinflation ○ Pneumothorax ○ Reduced venous return ● Permissive hypercapnia ○ Respiratory acidosis Ventilator settings ● Low RR ● Small Vt ● High peak inspiratory flow (70-100l/min) ● Prolonged expiratory time (I:E, 1:3 ● PEEP to compensate for PEEPi