3D Vision Syndrome
•
1 like•1,463 views

The 3D Vision Syndrome (3DVS) has all the required qualifications for a new but not yet officially recognized syndrome. A syndrome is comprised of a group of symptoms that collectively indicate or characterize a disease, psychological problem, other abnormal condition or, in this case, a functional vision disorder. 3DVS symptoms include headaches, blurred vision, eyestrain, diplopia, dizziness/nausea and motion sickness after watching a 3D movie, television or video game. This is the first report of an individual with 3DVS who has undergone optometric vision therapy (OVT). This poster will be presented at the American Academy of Optometry meeting in San Francisco this November. Please come to learn more about it!
Recommended

Recommended
More Related Content
What's hot
What's hot (19)
Similar to 3D Vision Syndrome
Similar to 3D Vision Syndrome (20)
More from Dominick Maino
More from Dominick Maino (20)
3D Vision Syndrome
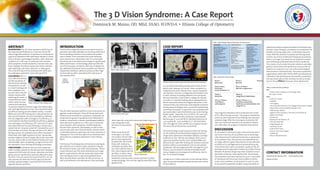
- 1. ABSTRACT BACKGROUND: The 3D Vision Syndrome (3DVS) has all the required qualifications for a new but not yet offi- cially recognized syndrome. A syndrome is comprised of a group of symptoms that collectively indicate or charac- terize a disease, psychological problem, other abnormal condition or, in this case, a functional vision disorder. 3DVS symptoms include headaches, blurred vision, eye- strain, diplopia, dizziness/nausea and motion sickness after watching a 3D movie, television or video game. This is the first report of an individual with 3DVS who has undergone optometric vision therapy (OVT). CASE REPORT: WS is a 27 y/o WF who present- ed with symptoms of blurred vision, diplopia, and eyestrain, as well as, visual tracking prob- lems, headache, nau- sea and vision induced motion sickness after watching 3D movies. A comprehensive exami- nation noted reduced random dot stereopsis, no positive/negative fusional ranges (immediate diplo- pia), and high exophoria at near. Also noted were diplo- pia while accessing accommodative facility, a variable MEM, pain upon NPC testing and a reduced positive rel- ative accommodation and accommodative amplitudes. She was diagnosed with convergence insufficiency, ac- commodative infacility/instability/insufficiency, diplopia and convergence insufficiency. OVT and home VT were prescribed with each session following a commonly ac- cepted format. Computer aided OVT included the use of Vision Builder and Home Therapy Solutions HTS. After 6 therapy sessions all symptoms were either improved or eliminated, with slight esophoria at near, measurable positive/negative fusional ranges, NPC to the nose with- out pain, measurable accommodative facility and a nor- malized MEM. Upon completing a program of out of of- fice optometric vision therapy all findings normalized. CONCLUSIONS: Individuals with 3D Vision Syndrome suffer multiple symptoms that decrease the individual’s enjoyment of the latest 3D movies, television and video games and can significantly adversely affect their qual- ity of life. This case report has shown that OVT can not only improve the abnormal clinical signs but also the multiple symptomologies associated with this techno- logically induced syndrome. INTRODUCTION The first technologically induced near-point visual im- pairment anomalies probably occurred around the time that Gutenberg started to mass produce the printed word in books. Once sustained near-point demands were required on a substantial scale, it is conceivable that binocular vision dysfunctions began to significantly affect performance. As technology advanced with the use of microscopes, computers and now 3 D digital me- dia, additional functional vision anomalies are noted to impede the individual’s ability to achieve at their high- est level and are often associated with a decrease in ones quality of life. The 3D Vision Syndrome (3DVS) is a true, but not yet rec- ognized, medical disorder. It has all the required quali- fications to be classified as a syndrome. Syndromes are comprised of a group of symptoms that collectively in- dicate or characterize a disease, psychological problem, other abnormal condition or, in this case, a functional vision disorder. 3DVS symptoms include headaches, blurred vision, eyestrain, and diplopia, as well as dizzi- ness/nausea and vision induced motion sickness which is intimately linked to watching a 3D movie, television or video game. This is the first report of an individual with 3DVS who has undergone optometric vision therapy (OVT). The history of technologically 3 dimensional viewing be- gan with the use of stereo-scopes invented in 1844 by the Scottish inventor and writer David Brewster. Stereo- scopic television was first demonstrated by John Logie Baird in 1928 while the first 3D movie that made head- lines was Bwana Devil in 1952 starring Robert Stack. More recently Avatar and other similiar 3D movies, as well as 3D television and video games, have seemingly burst upon the scene with comsumers beginning to ac- cept seeing their enter- tainment in three dimen- sions. While many of the 3D movie-goers, 3D Televi- sion viewers and 3D video- gamers have apparently accepted this new media, those with strabismus, amblyopia and other bioc- ular vision dysfunctions ei- ther cannot appreciate the 3D affect, or worse, leave the 3D environment with headachers, blurred vision, nausea, dizziness or other symportomology. This can then significantly affect their quality of life. CASE REPORT A 27 y/o W female (SW) presented with a host of com- plaints after viewing a 3D movie. These complaints in- cluded blurred vision, double vision, nausea, headache, and dizziness. She was a college educated athletic train- er with a history of reading problems since 5th grade. SW also informed us that while in college she needed to enroll in a remedial reading class to adequately han- dle the near point demands of higher educations. Here medical history was otherwise unremarkable except for having seasonal allergies and a successful nephrectomy and kidney transplant. A copy of her last comprehensive eye examination noted limited binocular vision testing, health “good”, aided VAs of 20/20 RE/LE, SLE unremark- able, a non-dilated fundus evaluation unremarkable, Retinoscopy of -4.00 Sph RE/LE, Manifest Refraction of -4.00-50X175 RE, -4.00-.50X180 LE, CT 2XO dist/Ortho near, BI vergences 20/8, and BO 24/12 vergence at near. She wore soft contact lenses successfully. The initial findings noted reduced random dot stereop- sis, the inability to elicited positive/negative fusional ranges (she experienced immediate diplopia), and high exophoria at near. SW was also diplopic when access- ing accommodative facility, had a variable MEM, com- plained of pain upon NPC testing and showed a reduced positive relative accommodation and accommodative amplitudes. SW was diagnosed with convergence insuf- ficiency, accommodative infacility/instability/insuffi- ciency, diplopia and convergence insufficiency. (See ta- ble 1 for all initial findings) A program of in office optometric vision therapy follow- ing a commonly excepted standard format was institut- ed. (see table 2). Two progress evaluations were conducted over a total of 8 in office therapy sessions. The progress evaluations noted not only improved clinical findings but improved symptomology. After the last progress evaluation SW saw a 3D movie and experience no symptoms whatso- ever. (See table 1 for progress evaluation information). DISCUSSION As 3D content continues to play a more and more domi- nant role in the lives of our patients and as technologi- cally induced visual impairments become a routine part of our patients’ lives, the primary care optometrist can no longer afford to ignore the presence of and detrimen- tal effects of an undiagnosed and untreated binocular vision dysfunction upon our patients’ quality of life. De- pending upon the population studied up to 56% of those between 18-38 years of age may show symptoms associ- ated with a binocular vision dysfunction. Accommoda- tive anomalies have been reported to occur in up to 80% of individuals with binocular vision problems and bin- ocular vision problems can be present in up to 20-30% of any specific population studied. Using commonly ac- cepted and evidence based modalities of treatment (op- tometric vision therapy), our patients can experience the benefits of having single, clear, comfortable, binocular vision. With the advent of computerized therapy tools and the use of more traditional therapeutic procedures, there is no longer any reason for our patients to experi- ence asthenopia associated with 3D Vision Syndrome. The creators of 3D content (movies, television and video- games) should work with optometry to ensure that all patients can enjoy this new 21st century technological advancement in entertainment. The various optometric organizations (AOA, AAO, COVD, OEPF) and educational institutions should emphasize the need for comprehen- sive eye examinations that routinely include an evalua- tion for the presence of binocular vision dysfunction. Table 3: Current and Future 3D Movies 2011 • Pirates of the Caribbean: on Stranger Tides The Green Hornet 2010 • Gulliver’s Travels • Yogi Bear • Tron Legacy • The Chronicles of Narnia: The Voyage of the Dawn Treader • Harry Potter and the Deathly Hallows: Part 1 • SAW 3D (aka: SAW 7) • Legend of the Guardians: The Owls of Ga’Hoole 3D • Alpha and Omega • Piranha 3D • Beauty and the Beast in 3D • The Last Airbender • King Kong 360 3D • Toy Story 3 in 3D • Clash of the Titans • How to Train Your Dragon • Hubble 3D • Alice in Wonderland 3D CONTACT INFORMATION Dominick M. Maino, OD dmaino@ico.edu www.ico.edu The 3 D Vision Syndrome: A Case Report Dominick M. Maino, OD, MEd, FAAO, FCOVD-A • Illinois College of Optometry 5 Table 1 Initial Findings Progress Evaluations Final Assessment Initial Findings VA’s CLS RE/LE 20/20 OR RE -.25, LE PL Acceptable Fit MR RE -4.25-50X175 20/15, LE -4.00-.50X175 20/15 Pursuits/Saccades +4 CT 18 XOP @ near 2nd Degree Fusion Variable Random Dot 100” (?) NPC 2/6/4” After 5 attempts pain noted PFV/NFV @ near could not do/diplopia - Lens amplitudes could not do NRA +2.00 diplopia PRA -1.00 Symptoms included blurred vision, double vision, nausea, headache, dizziness after viewing 3D content Final Progress Evaluation BVA 20/20 RE, LE Slight + CL OR CT ortho/2 EXO, NPC TN After 5 trials TN NPC with RL 7/10 cm Vergence dist BI x/14/10 BO X/30/25 Near BI 16/12 BO 35/25 W4D 4 all distances, Random Dot 25’ Pur/Sac +4 Amps 8.33 RE/LE NRA +2.50, PRA -2.25 Facility 6 RE, 7LE, 8 OU CPM no suppression MEM +.50 RE, LE Majority of symptoms resolved, saw 3D movie without any problems Total of 8 in office optometric vision therapy sessions and home therapy Progress Evaluation #1 20/15 BVA, RE/LE CL OR RE +1.00-.50X180 20/20 LE +1.25 20/20 MR RE -3.25-.25X175 20/20 LE -3.250.75X005 20/20 Pursuits +4 Saccades +3 CT 2EP (near) W4D 4 at all distances Random dot 20 ‘ NPC TN no pain BI 12/9 near BO > 45 Amps 7 D RE/LE Facility 8 CPM RE, 11 CPM LE, 10 CPM OU MEM +.75 each eye During evaluation no diplopia, pain, suppression, more stable findings. Symptoms improving, not completely resolved 5 Table 1 Initial Findings Progress Evaluations Final Assessment Initial Findings VA’s CLS RE/LE 20/20 OR RE -.25, LE PL Acceptable Fit MR RE -4.25-50X175 20/15, LE -4.00-.50X175 20/15 Pursuits/Saccades +4 CT 18 XOP @ near 2nd Degree Fusion Variable Random Dot 100” (?) NPC 2/6/4” After 5 attempts pain noted PFV/NFV @ near could not do/diplopia - Lens amplitudes could not do NRA +2.00 diplopia PRA -1.00 Symptoms included blurred vision, double vision, nausea, headache, dizziness after viewing 3D content Final Progress Evaluation BVA 20/20 RE, LE Slight + CL OR CT ortho/2 EXO, NPC TN After 5 trials TN NPC with RL 7/10 cm Vergence dist BI x/14/10 BO X/30/25 Near BI 16/12 BO 35/25 W4D 4 all distances, Random Dot 25’ Pur/Sac +4 Amps 8.33 RE/LE NRA +2.50, PRA -2.25 Facility 6 RE, 7LE, 8 OU CPM no suppression MEM +.50 RE, LE Majority of symptoms resolved, saw 3D movie without any problems Total of 8 in office optometric vision therapy sessions and home therapy Progress Evaluation #1 20/15 BVA, RE/LE CL OR RE +1.00-.50X180 20/20 LE +1.25 20/20 MR RE -3.25-.25X175 20/20 LE -3.250.75X005 20/20 Pursuits +4 Saccades +3 CT 2EP (near) W4D 4 at all distances Random dot 20 ‘ NPC TN no pain BI 12/9 near BO > 45 Amps 7 D RE/LE Facility 8 CPM RE, 11 CPM LE, 10 CPM OU MEM +.75 each eye During evaluation no diplopia, pain, suppression, more stable findings. Symptoms improving, not completely resolved 5 Table 1 Initial Findings Progress Evaluations Final Assessment Initial Findings VA’s CLS RE/LE 20/20 OR RE -.25, LE PL Acceptable Fit MR RE -4.25-50X175 20/15, LE -4.00-.50X175 20/15 Pursuits/Saccades +4 CT 18 XOP @ near 2nd Degree Fusion Variable Random Dot 100” (?) NPC 2/6/4” After 5 attempts pain noted PFV/NFV @ near could not do/diplopia - Lens amplitudes could not do NRA +2.00 diplopia PRA -1.00 Symptoms included blurred vision, double vision, nausea, headache, dizziness after viewing 3D content Final Progress Evaluation BVA 20/20 RE, LE Slight + CL OR CT ortho/2 EXO, NPC TN After 5 trials TN NPC with RL 7/10 cm Vergence dist BI x/14/10 BO X/30/25 Near BI 16/12 BO 35/25 W4D 4 all distances, Random Dot 25’ Pur/Sac +4 Amps 8.33 RE/LE NRA +2.50, PRA -2.25 Facility 6 RE, 7LE, 8 OU CPM no suppression MEM +.50 RE, LE Majority of symptoms resolved, saw 3D movie without any problems Total of 8 in office optometric vision therapy sessions and home therapy Progress Evaluation #1 20/15 BVA, RE/LE CL OR RE +1.00-.50X180 20/20 LE +1.25 20/20 MR RE -3.25-.25X175 20/20 LE -3.250.75X005 20/20 Pursuits +4 Saccades +3 CT 2EP (near) W4D 4 at all distances Random dot 20 ‘ NPC TN no pain BI 12/9 near BO > 45 Amps 7 D RE/LE Facility 8 CPM RE, 11 CPM LE, 10 CPM OU MEM +.75 each eye During evaluation no diplopia, pain, suppression, more stable findings. Symptoms improving, not completely resolved 6 Table 2 Optometric Vision Therapy Phase 1 Phase 2 Phase 3 Phase 4 Monocular Biocular Binocular Integration/Stabilization Oculo-motor, All as in Phase 1 All as in Phase 1 All as in Phase 1, 2, 3 Hand-eye, add anti-suppression and Phase 2 Combine oculomotor, accommodation Tx add vergence hand-eye, accommodation and vergence Tx 6 Table 2 Optometric Vision Therapy Phase 1 Phase 2 Phase 3 Phase 4 Monocular Biocular Binocular Integration/Stabilization Oculo-motor, All as in Phase 1 All as in Phase 1 All as in Phase 1, 2, 3 Hand-eye, add anti-suppression and Phase 2 Combine oculomotor, accommodation Tx add vergence hand-eye, accommodation and vergence Tx Photo 5: Bwana Devil Photo 6: Using the media to inform the public about 3D Vision Syndrome Table 1: Initial Findings, Progress Evaluations, Final Assessment Table 2: Optometric Vision Therapy Photo 3: Stereo television 1920s Photo 4: Stereo receiver 1920s Photo 2: Brewster stereoscope Photo 1: Binocular Vision Testing on SW