Mandana khalili aasld 2009 insulin secretion poster final
•Transferir como PPT, PDF•
1 gostou•680 visualizações

Dr. Mandana Khalili presensts on

Recomendados
Mais conteúdo relacionado
Destaque
Semelhante a Mandana khalili aasld 2009 insulin secretion poster final
Semelhante a Mandana khalili aasld 2009 insulin secretion poster final (18)
Mais de CTSI at UCSF
Mais de CTSI at UCSF (20)
Último
Último (20)
Mandana khalili aasld 2009 insulin secretion poster final
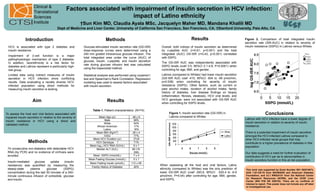
- 1. Clinical & Translational Factors associated with impairment of insulin secretion in HCV infection: Sciences impact of Latino ethnicity Institute †Sun Kim MD, Claudia Ayala MSc, Jacquelyn Maher MD, Mandana Khalili MD Dept of Medicine and Liver Center, University of California San Francisco, San Francisco, CA; †Stanford University, Palo Alto, CA UCSF Introduction Methods Results Figure 2. Comparison of total integrated insulin secretion rate (ISR-AUC) in relation to severity of HCV is associated with type 2 diabetes and Glucose-stimulated insulin secretion rate (GS-ISR) Overall, both indices of insulin secretion as determined insulin resistance (SSPG) in Latinos versus Whites insulin resistance. dose-response curves were determined using a by c-peptide AUC (r=0.61, p<0.001) and the total 240 min graded intravenous glucose infusion. The integrated (AUC) GS-ISR (r=0.43, p<0.001) correlated Impairment of -cell function is a major total integrated area under the curve (AUC) of with SSPG. pathophysiologic mechanism of type 2 diabetes. glucose, insulin, c-peptide, and insulin secretion The GS-ISR AUC was independently associated with In addition, race/ethnicity is a risk factor for rate during glucose infusion test was calculated SSPG levels (coef 3.5, 95%CI 2.1-4.8, P<0.0001) when diabetes and Latinos represent a particularly high- using the trapezoidal method. controlling for age, BMI, and gender. risk group. Limited data using indirect measures of insulin Statistical analysis was performed using unpaired t Latinos (compared to Whites) had lower insulin secretion secretion in HCV infection show conflicting test and Spearman’s Rank Correlation. Regression (GS-ISR AUC coef -410, 95%CI -834 to -69 pmol/min, results. Data evaluating a racially diverse HCV- modeling was used to assess factors associated p=0.038) when controlling for severity of insulin infected population using direct methods for with insulin secretion. resistance (SSPG). Other factors, such as current or measuring insulin secretion is lacking. past alcohol intake, duration of alcohol intake, family history of diabetes, liver disease findings on biopsy (inflammation, fibrosis, steatosis), HCV viral levels, and HCV genotype, were not associated with GS-ISR AUC Aim Results when controlling for SSPG levels. Table 1. Patient characteristics (N=74) To assess the host and viral factors associated with Figure 1. Insulin secretion rate (GS-ISR) in Conclusions impaired insulin secretion in relation to the severity of Mean Age (yr) 48 ± 9 Latinos compared to Whites Male 68% Latinos with HCV infection have a lower degree of insulin resistance in HCV using a direct and insulin secretion in relation to severity of insulin White 54% GS-ISR (pmol/min) validated method. 1200 African American 17% 1000 resistance. Latino 16% 800 Mean BMI (Kg/m2) 26 ± 4 White There is a potential impairment of insulin secretion 600 IVDU 77% Latino amongst the HCV-infected Latinos compared to 400 Mean HCV Duration (yr) 27±9 other HCV-infected racial groups that may Methods HCV Genotype 1 71% 200 contribute to a higher prevalence of diabetes in this Mean log10 HCV RNA (IU/mL) 6±1 0 population. 74 consecutive non-diabetics with detectable HCV Median ALT (IU/L) 68 (19- 5 6 7 8 9 RNA (by PCR) and no evidence of cirrhosis were 556) Glucose (mmol/L) Our data suggests a need for further evaluation of enrolled. Mean SSPG (mmol/dL) 7±4 contribution of HCV per se to abnormalities in Mean Fasting Glucose (mmol/L) 5±1 insulin secretory function in this at-risk population. Insulin-mediated glucose uptake (insulin Mean Fasting Insulin (pmol/L) 112 ± 69 resistance) was quantified by measuring the When assessing all the host and viral factors, Latino Family History of Diabetes 40% steady-state plasma glucose (SSPG) ethnicity (compared to Whites) was the only predictor of This work was supported by Grant Number R01 DK074673, concentration during the last 30 minutes of a 240- lower GS-ISR AUC (coef -263.6, 95%CI -520.4 to -6.9 ADA 1-07-CR-70 from NIH/NIDDK and American Diabetes minute continuous infusion of octreotide, glucose pmol/min, P=0.04) after controlling for age, BMI, gender, Foundation, and UL1 RR024131 from the National Center for Research Resources (NCRR), and the UCSF Liver and insulin. and SSPG. Center (NIH P30 DK 026743). There are no conflicts of interest to report. This poster does not include any off label or investigational use.