
Recomendados
Mais conteúdo relacionado
Último
Último (20)
Destaque
Destaque (20)
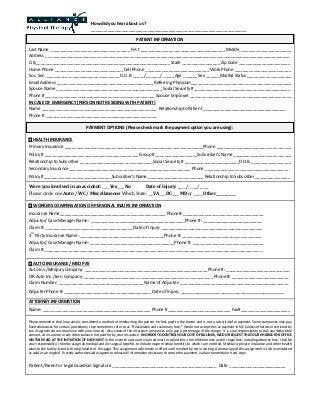
Alliance Physical Therapy : Registration_Form
- 1. Last Name __________________________________ First ____________________________________ Middle______________________ Address ________________________________________________________________________________________________________ City_________________________________________________________ State ________________ Zip Code ______________________ Home Phone _____________________________ Cell Phone ___________________________ Work Phone ________________________ Soc. Sec. _______________________________ D.O.B _____/______/_____ Age ______ Sex ______Marital Status___________________ Email Address _________________________________________ Referring Physician___________________________________________ Spouse Name _____________________________________________ Social Security #_________________________________________ Phone #_______________________________________________ Spouse Employer ___________________________________________ IN CASE OF EMERGENCY (PERSON NOT RESIDING WITH PATIENT) Name _________________________________________________ Relationship to Patient ___________________________________ Phone # _______________________________________________ HEALTH INSURANCE PrimaryInsurance ___________________________________________________________Phone ________________________________ Policy # ________________________________________ Group# __________________Subscriber’s Name_________________________ Relationship to Subscriber _______________________________Social Security # _______________________D.O.B._________________ Secondary Insurance____________________________________________________ Phone____________________________________ Policy #_____________________________Subscriber’s Name________________________ Relationship to Subscriber_______________ Were you involved in an accident: ____Yes____ No Date of Injury: _____/_____/_____ Please circle one Auto / WC / Miscellaneous Which State: ___VA____DC____ MD or _____ Other___________ WORKERS COMPENSATION OR PERSONAL INJURY INFORMATION Insurance Name_____________________________________________ Phone#: __________________________________ Adjustor/ Case Manager Name: ________________________________________Phone #: _________________________ Claim #: _____________________________________ Date ofInjury: ___________________________________________ 3 rd PartyInsurance Name:____________________________________Phone #:__________________________________ Adjustor/ Case Manager Name: ____________________________________Phone #: ______________________________ Claim #:_____________________________________________________________________________________________ AUTO INSURANCE/ MED PAY AutoIns./Medpay Company: ____________________________________________________ Phone #: ___________________________ OR Auto Ins./Lien Company: _______________________________________________________ Phone #: ________________________ Claim Number: ____________________________________ Name of Adjuster: ______________________________________________ Adjuster Phone #: _____________________________________ Date ofInjury: ____________________________________ ATTORNEY INFORMATION Name: ______________________________________________ Phone #___________________________ Fax#_____________________ Please remember that Insurance is considered a method of reimbursing the patient for fees paid to the doctor and is not a sub stitute for payment. Some companies may pay fixed allowances for certain procedures; they sometimes ref er to as “Reasonable and customary fees.” We do not accept this as payment in full (unless otherwise restricted by law or agreement we may have with your insurer). Also some of the insurance companies only pay a percentage of the charge. It is your responsibility to pay any deductible amount, co-insurance or any other balance not paid for by your insurance. IN ORDER TO CONTROL YOUR COST OF BILLINGS, WE DO REQUEST THAT OUR CHARGE FOR OFFICE VISITS BE PAID AT THE INITIATION OF EACH VISIT. In the event the account is turned over for collections, the collection fees and /or legal fees, including attorney fees, s hall be your responsibility. I hereby assign all medical and/or surgical benefits to include major medical benefits to which I am entitled, Medicare, private insurance and other health plans to the facility listed in the top header of this page. This assignment will remain in effect until revoked by me in writing. A photocopy of this assignment is to be considered as valid as an original. I hereby authorize said assignee to releas e all information necessary to secure the payment, via fax transmittal or hard copy. Patient/Parent or Legal Guardian Signature ____________________________________________ Date ________________________ How did you hear about us? __________________________________________________________________ PAYMENT OPTIONS (Please check mark the payment option you are using): PATIENT INFORMATION