Call Girls Dehradun Just Call 9907093804 Top Class Call Girl Service Available
8 Lower Respiratory Infections
1. Bronchiolitis
Bronchitis
Pneumonia
Acute
Chronic
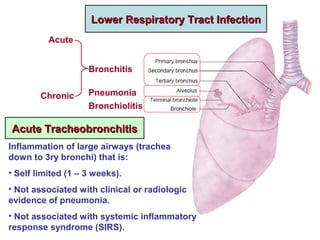
Lower Respiratory Tract InfectionLower Respiratory Tract Infection
Acute TracheobronchitisAcute Tracheobronchitis
Inflammation of large airways (trachea
down to 3ry bronchi) that is:
• Self limited (1 – 3 weeks).
• Not associated with clinical or radiologic
evidence of pneumonia.
• Not associated with systemic inflammatory
response syndrome (SIRS).
2. • SIRS: > 2 criteria of:
- Temp > 38 O
C.
- Pulse > 90 b/min.
- RR > 20 b/min.
- WBCs > 12,000 cells/mm3
.
• Epidemiology:
- Affects > 5% of adults annually.
- More in cold season.
- Viral in most cases, but usually empirically treated with antibiotics.
• Treatment:
- Rest, expectorants, mucolytics, antipyretics.
- Antimicrobials if indicated:
o Antibiotics: Azithromycin 500 mg tab once daily for 3 days.
Or Doxycycline 100 mg/12 h for 5 days.
o Antivirals: Oseltamivir (Tamiflu) tab 75 mg twice daily for 5 days
(during seasonal outbreaks of influenza).
3. Pneumonitis
Pneumonia
Pneumonitis: broad term for inflammation of the lung.
Pneumonia: used more specifically to indicate inflammation of lung
parenchyma which is:
• Caused by an infectious agent.
• Leads to formation of an inflammatory exudate inside the alveoli.
• Leads to loss of aeriation of lung tissue.
This is referred to as hepatization (pathology) or consolidation (clinical).
(Patchy) (Confluent)
4. Clinical Types of Pneumonia
• Health Care Associated Pneumonia (HCAP): Diagnosed if the
patient:
- Was hospitalized for > 2 days within the last 3 months.
- Lives in a nursing facility.
- Was repeatedly exposed to a medical facility (hemodialysis, wound
care, IV antibiotics or chemotherapy)
• Hospital Acquired Pneumonia (HAP)
(Nosocomial Pneumonia): develops:
- > 48 hh after hospitalization (not incubating at time of admission).
- Soon after discharge from hospital.
- Ventilator Associated Pneumonia (VAP): a subtype of HAP: It develops
> 48 hh after start of mechanical ventilation.
• Community Acquired Pneumonia (CAP): acquired outside the
above circumstances (unrelated to healthcare).
5. Epidemiology
• Commonest potentially lethal acute infection.
• A leading type of nosocomial (hospital- acquired) infection.
• Commoner and more risky at extremes of age (< 2, > 65 y).
• CAP is commonly preceded by a viral respiratory tract
infection →
o ↑ Adherence of bacteria to respiratory epithelial cells.
o ↓ Mucociliary clearance.
• HAP is responsible for 25% of ICU admissions.
• VAP is the most frequent ICU acquired infection.
• Aspiration pneumonia may be community or hospital
acquired, though it more typically occurs in hospitals or
extended care facilities.
6. Community Acquired Pneumonia (CAP)Community Acquired Pneumonia (CAP)
Route of Infection• Microaspiration
Unrecognized microaspiration is the usual route of
infection for typical CAP caused by S. pneumoniae and H.
influenzae. Some degree of microaspiration normally
occurs during sleep. If upper airways are colonized or
infected, small amounts of oral or pharyngeal secretions
that are aspirated will carry the bacteria to the alveoli
where they trigger the pneumonic process.
• Inhalation as in transmission of:
- Viral pneumonia.
- Tuberculosis.
• Haematogenous Spread as in Staph. aureus pneumonia.
• Direct Extension from pleura or subdiaphragmatic space.
7. Microorganisms
Common
• Streptococcus pneumoniae
(pneumococci): commonest
and most typical.
• Haemophylus influenzae.
• Influenza virus, other
respiratory viruses
• Satphylococcus aureus
• Mycobacterium
tuberculosis
Less Common
• Moraxella catarrhalis.
• Pseudomonas aeroginosa.
• Klebsiella.
• Mycoplasma.
• Chlamydia (C. pneumoniae
and C. psittaci)
• Legionella.
• Fungi
Atypical organisms as Mycoplasma, Chlamydia, fungi
are not revealed by ordinary Gram stain and culture.
8. Predisposing Conditions for Particular Organisms
• Smoking, COPD predispose to CAP with typical
organisms (S. pmeumoniae, H. influenzae, M. catarrhalis)
as well as P. aeroginosa.
• P. aeroginosa is predisposed to by structural lung
damage as in bronchiectasis, cystic fibrosis.
• S. aureus is predisposed to by:
o Viral infection.
o IV drug abuse.
o Endovascular infection as endocarditis.
o Chronic renal failure.
• Cavitary lung lesions may denote
S. aureus, Klebsiella or tuberculosis.
9. • Dental problems and poor oral hygiene predispose to
infection with anaerobic organisms.
• Exposure to birds predisposes to infection with
C. psittaci (psittacosis).
• HIV predisposes to:
- Pneumocystis jirovecii pneumonia (PJP)
(formerly Pneumocystis carinii pneumonia (PCP)
- Tuberculosis
- P. aeroginosa.
- Fungal infection
• Asplenia (anatomic or functional) predisposes to invasive
infections with encapsulated organisms
(pneumococci, meningococci, Klebsiella).
10. Clinical Picture
Typical Pneumonia
• Fever, malaise.
• Cough with little (rusty) sputum.
• Pleuritic chest pain.
• Dyspnoea.
Atypical Pneumonia
• Elderly: Confusion and subtle changes of mental status
dominate the picture.
• Viral pneumonia: upper respiratory symptoms as
rhinorrhoea, sore throat, dry cough. It occasionally occurs
in epidemics or even pandemics (avian flu, swine flu)
• Atypical organisms (Mycoplasma, chlamydia): more
insidious onset, subtle symptoms (walking pneumonia).
11. InvestigationsChest X-Ray
• Typical: unilateral lobar or segmental consolidation
• Atypical:
o Radiographic infiltrates that are not clearly segmental.
o Small areas of alveolar consolidation may be missed, esp. in AP
portable radiographs (but detected by the far more sensitive CT).
o Rapidly progressive pneumonia of any cause may produce
diffuse pulmonary infiltrates consistent with ARDS.
Culture
• Respiratory sample:
o Sputum (spontaneous or induced by saline inhalation)
o Endotracheal aspiration.
o Bronchoalveolar lavage (BAL).
Specimens obtained from lower respiratory tract are more predictive
of true infection rather than colonization.
13. • Blood: Bacteraemia may be documented in:
- 10% of patients hospitalized for CAP.
- Most patients with haematogenous S. aureus pneumonia.
C-Reactive Protein may be a useful indicator of the extent of
parenchymal inflammation in pneumonia. It may also be utilized to
assess the response to treatment.
Lobar Pneumonia, Right Middle Lobe
14. C Confusion 1
U BUN > 20 mg/dL 1
R Respiratory Rate > 30 b/min 1
B BP < 90/60 mmHg or need
for fluid resuscitation
1
65 Age > 65 y 1
CURB-65 score ranges 0 – 5
CRB-65 score ranges 0 – 4
(BUN excluded).
Urea : Urea nitrogen = 60 : 28 (30 : 14)
0
10
20
30
40
50
60
0 1 2 3 4 5
CAP Mortality %
In Relation to CURB-65 Score
CURB-
65 Score
CAP
Severity
Initial
Treatment
0 – 1 Mild Out- patient
2 – 3 Moderate Out- or In-
patient
4 - 5 Severe In- patient,
possibly
ICU
CAP Severity Scores
15. This means persistence of pulmonary infiltrates > 30 days after initial
presentation.
• Causes:
• Resistant organism.
• Missed organism (TB / fungus).
• Nosocomial superinfection: another pneumonia, empyema, endocarditis
• Non- infectious complications: eg, Bronchiolitis Obliterans Organizing Pneumonia.
Non-Resolving or Slowly Resolving Pneumonia
Bronchiloitis Obliterans Organizing Pneumonia (BOOP)
• Comorbidities: DM, RF, HF
• Immunocompromised states
Resolution of pneumonia requires resorption of the inflammatory exudate in
the alveoli. In BOOP, the inflammatory exudate persists in the alveoli and
bronchioles and becomes organized into fibrous tissue which further
obliterates the air spaces.
X-Ray shows bilateral wide spread patches of fibrosis.
Diagnosis is confirmed by CT and bronchoscopic biopsy.
Most patients recover with steroid therapy.
16. Complications
• Empyema: most common infectious complication
It should be considered in patients with persistent fever and leucocytosis
after 4 – 5 days of appropriate antibiotic treatment.
• Extra- Pulmonary Infection eg, arthritis, osteomyelitis, endocarditis.
• VTE (Venous Thromboembolism)
Risk ↑ at both short and long term but is highest in the 4 weeks following
diagnosis.
Pneumococcal infection has been specifically associated with host
thrombotic tendency stimulated by components of the bacterial cell wall.
• BOOP Mortality
< 1%: in outpatient treated CAP
> 10%: in hospitalized patients
40%: in ICU patients
Influenza vaccination ↓ risk of influenza and all cause pneumonia.
17. Treatment of CAP
- Rest, expectorants, mucolytics, antipyretics.
- Good hydration, may entail IV fluids.
- Airway clearance techniques (respiratory therapy).
- Prophylactic anticoagulation in hospitalized patients. Low molecular weight
heparin should be considered in all patients who are not fully mobile.
- Oxygen therapy as guided by oximetry.
- Duration of treatment:
• Outpatient, not complicated: 5 – 7 days.
• Hospitalized: initial IV then oral treatment for a total of 7 – 10 days.
• Non- Bacteraemic invasive organisms (as Staph. Aureus, Gm –ve
bacilli): IV treatment for 10 to 14 days.
• Bacteraemic Staph. aureus: 4 weeks of IV therapy because of organism
resistance and the possibility of infective endocarditis as a cause or
a consequence of pneumonia.
• Atypical pneumonia: 2 weeks
• PJP: 3 weeks
• Fungal pneumonia: several months
18. Indications for Hospital Admission
• CURB-65 score > 2.
• Septic shock with need for
vasopressors (ICU required).
• Need for mechanical ventilation
(ICU required).
• Need for non- invasive
ventilation.
• PaO2 / FiO2 < 250 mmHg
(acute lung injury).
• Hypothermia < 36 O
C.
• Comorbidities, eg ESRD, ACS.
• Inability to take oral medicines.
• No responsible care giver.
• Failure of out- patient treatment.
Indications for Discharge
(Clinical Stability)
• Afebrile for > 48 hh.
• Haemodynamically stable
without vasopressors.
• No tachypnoea.
• No hypoxaemia
(SaO2 > 90% on room air).
• Normal mental status.
• Normally functioning GIT.
(so the patient can be given oral
medications)
19. Empiric Antibiotic Treatment
• Assessment (CURB – 65 score and other parameters) will dictate
whether treatment is initiated orally as outpatient, or parenterally as
inpatient.
• Moderate cases may be started on IV antibiotics to be shortly converted
to an oral regimen.
Outpatient Treatment
Mild Cases
Amoxiclav remains the drug of choice: tab 1 gm / 12hh for 5 – 7 days.
Alternatives if allergic to penicillin:
• Macrolide as Azithromycin tab 500 mg daily for 3 – 5 days
• Tetracycline as Doxycycline cap 100 mg / 12 hh for 7 days
• Quinolone as Levofloxacin tab 500 mg or Moxifloxacin tab 400 mg once
daily.
Moderate Cases
Amoxiclav + Macrolide Treatment may be initiated parenterally.
20. Inpatient Treatment for Severe cases; treatment is started IV:
[β-Lactam + Macrolide] Or Quinolone
β-Lactam as
Amoxiclav 1.2 gm/12h
Ampicillin/Sulbactam 1 gm/8h
Cefotaxime 1 gm/6h
Cetriaxone 1 gm/12h
Macrolide as
Azithromycin 500 mg/day
Quinolone as
Levofloxacin 750 mg/day
Moxifloxacin 400 mg/day
In case of parenteral cephalosporins, oral
switch is preferably made to oral amoxiclav
rather than oral cephalosporins
Respiratory fluoroquinolones are generally effective
for empirical therapy of CAP.
They are ideal for IV to oral shift (same dose).
21. Pseudomonas aeroginosa
Anti-Pseudomonal β-Lactam
• Piperacillin / Tazobactam 4.5 gm IV /6h
• Ceftazidime 1 gm IM/IV /8h
• Cefepime 2 gm IV /12h
• Imipenem / Cilastatin 1 gm IV /8h
• Meropenem 1 gm IV /8h
Antibiotics for Specific Pathogens
Extended infusion of carbapenems
may be preferable
Klebsiella & Acinetobacter
Carbapenem (Imipenem or Meropenem)
If resistant: Colistin (Polymixin E) 2.5 – 5 mg/kg/day IV in 3 divided doses
1 mg Colistin Base = 3000 IU
There are various forms of colistin used for inhalation therapy (eg. dry
powder for inhalation, solution for nebulization). This minimizes
nephrotoxicity from systemic absorption.
23. Mycoplasma &
Chlamydia
Doxycyclin cap 100 mg PO/12h
Or Macrolide (Azithromycin or Clarithromycin)
Treatment for 14 days
Legionella Fluoroquinolones for 14 days, starting IV then
shifting to oral.
PJP
(Pneumcystis
Jirovecii
Pneumonia)
Trimethoprim / Sulphamethoxazole 15 mg
TMP/Kg/day IV Div /8h or 2 DS tablets (800 mg
sulfamethoxazole and 160 mg trimethoprim) PO /
8h for 21 days
Fungal
Pneumonia
(Aspergillosos,
Histoplasmosis)
Itraconazole 200 mg PO or IV q24h
Or Amphotericin B 3 mg/kg q24h if severe
Duration of therapy: 1-12 months
24. Aspiration Pneumonitis / PneumoniaAspiration Pneumonitis / Pneumonia
Aspiration is defined as inhalation of oropharyngeal or gastric
contents into the larynx and lower respiratory tract.
Aspiration Pneumonitis is a chemical injury caused by aspiration of
sterile gastric contents.
Aspiration Pneumonia is an infectious process caused by aspiration
of oropharyngeal secretions colonized or infected by pathogenic
bacteria.
However, it is difficult in practice to distinguish between infectious
and non- infectious aspiration pneumonia. Aspiration should be
initially considered as infectious and treated as such.
Pulmonary aspiration is an important cause of serious illness and
death among residents of nursing homes and hospitalized patients.
However, many aspiration events probably pass unrecognized and
are not adequately treated.
Aspiration pneumonia is a common cause of death in patients with
neurologic dysphagia.
25. Predisposing Factors
For Occurrence of Aspiration
• Diminished gag and cough
reflexes due to: anaesthesia, CNS
depressants, stroke, dementia, old
age, asthenia. Post- extubation is
a very vulnerable period.
• Poor glottal function.
• Seizures.
• Choking while vomiting.
• Severe GERD.
• Mechanical ventilation: One of
the most common risk factors for
HAP. Ventilation and related
interventions (intubation,
sedation) ↑ risk of oropharyngeal
and gastric aspiration.
For the Aspirate to Contain
Bacteria
Oropharyngeal Aspirate
• Upper respiratory infection.
• Poor dental hygiene
Gastric Aspirate
• Hypo/Achlorhydria: as in patients
given PPIs or H2 blockers for
stress bleeding prophylaxis.
Sucralfate (Gastrofait) does not
↑ risk of pneumonia.
• Gastroparesis.
• Intestinal obstruction.
26. Organisms
Usually polymicrobial because oropharyngeal secretions contain
massive numbers of different organisms (aerobic, anaerobic).
Prevention
• Dietary Education
• Eat only while sitting and fully awake.
• Eat slowly, soft food, small bite size.
• Swallow slowly and repeatedly.
• Good Oral Hygiene
• Tube Feeding (NGT or Gastrostomy): may be used in patients with
poor cough and gag reflexes. Gastrostomy tube is better than NGT
regarding delivery of prescribed nutrition, but it does not prevent
gastric aspiration. Aspiration pneumonia is the commonest cause of
death in patients fed with gastrostomy tube. Both tubes offer no
protection against oropharyngeal aspiration.
• Endotracheal Intubation: to protect the airways in patients with low
level of consciousness.
27. Treatment of Aspiration Pneumonia
IV antibiotics are given for 7 – 10 days.
If cavitation is present, they may be continued for several weeks.
Options include:
• Piperacillin / Tazobactam 4.5 gm / 8h.
• Ceftazidime 2 gm / 8h.
• Ceftriaxone 1 gm / 12h.
• Levofloxacin 500 mg / day.
Add coverage for anaerobes in case of severe periodontal disease,
putrid sputum, evidence for necrotizing pneumonia or lung abscess:
• Clindamycin 600 mg / 8h. Or
• Metronidazole 500 mg / 8h.
NB: Corticosteroids were used for decades, but there is no evidence of
benefit.
28. Hospital Acquired Pneumonia (HAP)Hospital Acquired Pneumonia (HAP)
• If occurs within 4 days of hospital admission, organisms
are relatively antibiotic susceptible. Later onset HAP is
frequently caused by multi- drug resistant organisms
(MDROs) and may be polymicrobial.
• Most commonly identified organisms:
S. aureus, P. aeroginosa.
• High mortality, approaching 30 – 50% due to:
o Severity of pneumonia.
o Difficulty in providing antibiotic coverage.
o Underlying diseases and comorbidities.
29. Ventilator Associated Pneumonia (VAP)Ventilator Associated Pneumonia (VAP)
• Diagnosis is difficult because of the subjective nature of
the variables considered (nature of respiratory secretions
and CXR infiltrates) and the presence of many alternative
explanations (ARDS, atelectasis, pulmonary embolism,
heart failure,…)
• Even if organisms are cultured from respiratory
secretions, it remains difficult to determine whether they
represent true infection or mere colonization.
• Mortality rates and health care costs are among the
highest among all HAIs and among all HAPs.
30. Prevention of VAP
• Avoiding mechanical ventilation is the most effective
preventive measure. Non- invasive ventilation may be used
instead.
• Proper sterilization of the ventilator.
• Daily assessment of readiness for weaning from ventilator.
• Daily “sedation vacation”, if possible.
• Elevation of head of bed.
• Regular mouth care.
• Regular aspiration of subglottic secretions.
• Prohibition of unnecessary PPIs and H2 blockers use.
• Selective oropharyngeal and/or digestive tract
decontamination has been associated with significant
reduction in VAP, but may lead to selection of MDROs.
Notas do Editor
Colonization refers to presence of bacteria at some body site without causing inflammation or tissue destruction, on the contrary to infection which indicates that bacteria are causing some local or systemic harm.
Identification of influenza virus in a patient with pneumonia should lead to appropriate antiviral treatment, even if &gt; 48 hours passed since the onset of symptoms.