Acyanotic congenital heart diseases
•
15 gostaram•3,486 visualizações

Acyanotic congenital heart diseases VSD ASD AVSD PDA

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Acyanotic congenital heart diseases
Semelhante a Acyanotic congenital heart diseases (20)
Mais de Yapa
Mais de Yapa (20)
Último
Último (20)
Acyanotic congenital heart diseases
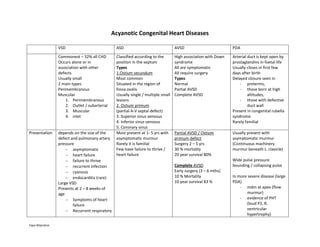
- 1. Yapa Wijeratne Acyanotic Congenital Heart Diseases VSD ASD AVSD PDA Commonest – 32% all CHD Occurs alone or in association with other defects Usually small 2 main types Perimembranous Muscular 1. Perimembranous 2. Outlet / subarterial 3. Muscular 4. inlet Classified according to the position in the septum Types 1.Ostium secundum Most common Situated in the region of fossa ovalis Usually single / multiple small lesions 2. Ostium primum (partial A-V septal defect) 3. Superior sinus venosus 4. Inferior sinus venosus 5. Coronary sinus High association with Down syndrome All are symptomatic All require surgery Types Normal Partial AVSD Complete AVSD Arterial duct is kept open by prostaglandins in foetal life Usually closes in first few days after birth Delayed closure seen in - preterms, - those born at high altitudes, - those with defective duct wall Present in congenital rubella syndrome Rarely familial Presentation depends on the size of the defect and pulmonary artery pressure asymptomatic heart failure failure to thrive recurrent infection cyanosis endocarditis (rare) Large VSD Presents at 2 – 8 weeks of age Symptoms of heart failure Recurrent respiratory Most present at 1- 5 yrs with asymptomatic murmur Rarely it is familial Few have failure to thrive / heart failure Partial AVSD / Ostium primum defect Surgery 2 – 5 yrs 30 % mortality 20 year survival 80% Complete AVSD Early surgery (3 – 6 mths) 10 % Mortality 10 year survival 83 % Usually present with asymptomatic murmur (Continuous machinery murmur beneath L. clavicle) Wide pulse pressure bounding / collapsing pulse In more severe disease (large PDA) - mdm at apex (flow murmur) - evidence of PHT (loud P2, R. ventricular hypertrophy)
- 2. Yapa Wijeratne infection Tachypnoea / dyspnoea Intercostal / subcostal recessions With PHT – symptoms↓ develops cyanosis (Eisenmenger’s) - Eisenmenger’s - late Precordial findings psm+ maximum at L. parasternal region mdm at apex (flow murmur) gallop rhythm Loud P2 Delayed P2 & fixed splitting of 2nd heart sound Systolic murmur at pulmonary area (increased flow) DD 1. Venous hum Varies with posture / head movement Best heard on right side 2. AV malformation Coronary, chest-wall, pulmonary 3. VSD with aortic regurgitation 4. Ruptured sinus of Valsalva aneurysm ECG biventricular hypertrophy (in PHT) Upright “T” wave in V1 in PHT incomplete RBBB > 90 % (10 % normal will also have RBBB) R axis deviation CXR Cardiomegaly Enlarged pulmonary arteries Peripheral pruning Increased hilar vascular markings Pulmonary oedema. Cardiomegaly Enlarged pulmonary arteries Pulmonary plethora Cardiomegaly Enlarged pulmonary arteries Peripheral pruning Pulmonary plethora Prognosis > 2/3 of muscular defects & 1/3 of perimembranous defects - close spontaneously within
- 3. Yapa Wijeratne 6 yrs. Management Small VSD with normal pul. artery pressure review regularly antibiotic prophylaxis for SABE long term survival is excellent Large VSD with symptoms Treat heart failure NG feeding + added calories Surgery If primary repair not possible - pulmonary artery banding Surgery for VSD Indications for surgery within first year 1. severe symptoms with failure to thrive 2. PHT If pul. Artery pressure > 75% of systemic pressure surgery in 2nd year Large VSD with pulmonary : systemic flow ratio > 2 : 1 surgery in 4-5 yrs. Operative mortality < 5 % long term survival - excellent Spontaneous closure is unusual Defects < 6 mm may close spontaneously in the neonatal period Defects > 8 mm in diameter unlikely to close Surgery recommended from the age of 2 yrs. (usually before school age) Bacterial endocarditis very rare Transcatheter procedure It is possible to close central defects by using varies devices Low risk High closure rates Surgical closure Direct suture / patch < 1 % mortality 10 % post-cardiotomy syndrome with pericardial effusion Survival similar to that of general population Fluid restriction / diuretics Indomethacin – in neonates Transcatheter closure Method of choice Occlusion rate > 98 % Surgical ligation for large defects Mortality < 0.5 % Outcome is excellent Risk of recurrent laryngeal nerve palsy, recanalization, inadvertent ligation of L. pulmonary artery