Recomendados

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (19)
Semelhante a Forehead Reconstruction Using a Modified A to T Dual Plane Flap
Semelhante a Forehead Reconstruction Using a Modified A to T Dual Plane Flap (10)
Mais de W. Thomas McClellan, MD FACS
Mais de W. Thomas McClellan, MD FACS (20)
Último
Último (20)
Forehead Reconstruction Using a Modified A to T Dual Plane Flap
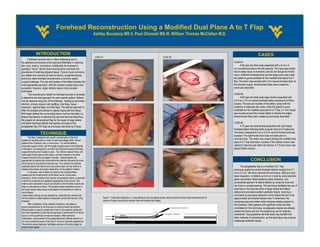
- 1. Forehead Reconstruction Using a Modified Dual Plane A to T Flap Ashley Boustany MS II, Paul Ghareeb MS III, William Thomas McClellan M.D. INTRODUCTION CASES CASE #1: CASE #2: Forehead reconstruction is often challenging due to the aesthetic prominence of the area and difficulties in matching CASE #1: skin color, contour, and texture. Additionally the forehead is A 62 year old white male presented with a 6 cm x 6 typically a “donor” site for facial reconstruction and lacks the cm neurofibroma above the left eyebrow. The mass was mobile, abundance of matching adjacent tissue. Tumors (most commonly had no deep tissue involvement, and did not disrupt the frontal sun related skin cancers) as well as trauma, congenital lesions, nerve. Sufficient forehead laxity and the large tumor size made and burns make forehead reconstruction a common plastic the patient a good candidate for the modified dual plane A to T surgical challenge. The size and location of the defect dictates the flap. The lesion was excised with 3 mm around all sides down to most appropriate approach, with the simplest usually being most the frontalis muscle. Advancement flaps were created as successful. However, larger defects require more complex previously described. techniques. The reconstructive ladder for forehead wounds is reviewed CASE #2: to determine the best approach for each specific patient. Defects A 68 year old white male cigar smoker presented with may be repaired using any of the following: healing by secondary a 4.0 cm x 4.0 cm central forehead defect resulting from Mohs intention, primary closure, skin grafting, local flaps, tissue surgery. The size and location of the defect, along with the expansion, regional flaps, and free flaps. The optimal approach is presence of adequate skin laxity, made the patient a good often the simplest and strives to replace tissue with like tissue. candidate for the modified dual plane A to T flap. A 1 mm margin With larger defects the surrounding tissue must be recruited in a was excised around the circular defect to freshen the edges. tension free fashion to optimize the scar and terminal blood flow. Advancement flaps were created as previously described. We present an advancement flap for the repair of large central and lateral forehead defects that applies principles of the CASE #3: periglabellar flap (PIG flap) as previously described by Chang. A 73 year old white female presented with right lateral forehead defect following Mohs surgical removal of melanoma. TECHNIQUE The lesion measured 8.0 cm x 5.0 cm and the frontal bone was exposed. The right frontal nerve was not intact prior to The flap is designed with careful consideration of the final reconstruction. The defect was closed utilizing the modified dual location of resulting scars in order to best camouflage within natural relaxed lines of tension, hair, or brow lines. For central defects, plane A to T flap described. Z-plasty of the vertical incision was horizontal superior limbs, with the length roughly equal to the diameter utilized to hide the scar within the hairline. A 7-French drain was of the lesion, are designed to lie within the natural transverse forehead placed before closure. crease formed by the frontalis muscle. Two inferior vertical limbs, with width equal to the radius of the lesion, are then marked to lie within creases formed by the corrugator muscles . Lateral defects are approached by placing the horizontal limbs inferiorly following the brow CONCLUSION which serves to conceal the eventual scar. The vertical limb extends cephalad toward the hairline and can extend back into the hairline or The periglabellar flap is a modified A to T flap chased transversely at its apex depending on the patient’s hairline. previously applied to central forehead defects ranging from 2.1 In all cases, care is taken to preserve the supratrochlear cm to 5.3 cm. We have improved this technique, utilizing a dual vessels and the frontal branch of the facial nerve. A dual plane plane dissection, to defects up to 8 cm in size by using extended dissection, which consists of an anterior and posterior plane, is essential galea recruitment, liberal posterior plane dissection, and to both the functional and aesthetic appearance of the wound. The anterior plane dissection occurs just anterior to the frontalis muscle and successfully applied it to lateral defects by using the brow and deep to subcutaneous tissue. The posterior plane dissection occurs in hair lines to conceal scarring. This technique facilitates the use of the loose areolar tissue deep to the galea in all directions in order to local flaps in the reconstruction of large central and lateral recruit tissue. defects and provides excellent aesthetic results. Scarring is Lateral defect closure can be assisted by extending the vertical limb minimized by dual plane dissection which allows the skin to be into the hairline to allow additional dissection across the horizon of the Figure 1: Dual plane dissection, in subcutaneous and sub-galeal planes, allows optimal en-bloc tissue advancement for approximated and exerted tension-free. Furthermore, the forehead. closure of larger wounds plus tension free and everted skin edges. remaining scars are hidden within features already present on After completion of the posterior dissection, the galea is the forehead. Older patients with significant laxity are ideal scored perpendicular to the long axis to improve tissue recruitment. candidates for this technique, as adequate creases are already Electrocautery is used to create short rents in the posterior galea and present and brow and hair line positioning can be relatively then blunt separation to the intervening tissue is performed to minimize injury to more superficial nerves and vessels. After extensive maintained. Young patients with little laxity may benefit from mobilization, advancement of the galea effectively offloads tension on other methods of reconstruction, as this technique may produce the more superficial layers of the skin to improve cosmetic appearance. inadequate aesthetic results. The anterior plane dissection facilitates eversion of the skin edges to improve scar quality. POSTER TEMPLATE BY: www.PosterPresentations.com