1. cva or stroke
•Download as PPSX, PDF•
33 likes•8,372 views


Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to 1. cva or stroke
Similar to 1. cva or stroke (20)
More from BP KOIRALA INSTITUTE OF HELATH SCIENCS,, NEPAL
More from BP KOIRALA INSTITUTE OF HELATH SCIENCS,, NEPAL (20)
Recently uploaded
Recently uploaded (20)
1. cva or stroke
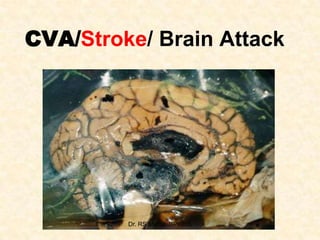
- 1. CVA/Stroke/ Brain Attack Dr. RS Mehta, BPKIHS
- 2. • C V A common : middle or late years of life. • Incidence ↑ With age. • Now referred to as strokes or brain attacks • Acute and treatable condition • Third leading cause of death in Developed Countries. • Leading cause of disability Dr. RS Mehta, BPKIHS
- 3. Brain Blood Supply • • • • Brain 2% of body weight 15-20% of Cardiac output 20% of Total body oxygen Neurons: predominantly Aerobic Dr. RS Mehta, BPKIHS
- 4. Dr. RS Mehta, BPKIHS
- 5. Dr. RS Mehta, BPKIHS
- 6. Circle of wills Dr. RS Mehta, BPKIHS
- 7. Dr. RS Mehta, BPKIHS
- 8. • A stroke is a clinical syndrome consisting of group of neurologic findings. • Cerebrovascular accident (CVA/stroke) is the infarction (death) of brain tissue caused by the disruption of blood flow to the brain. • It is characterized by focal neurological deficits specific to the area of the brain involved. Dr. RS Mehta, BPKIHS
- 9. Classification: • Transient ischemic attack (TIA) (<24). • Reversible ischemic neurologic deficit (RIND). (complete >24 hrs) • Partial non-progressing stroke (PNS). • Progressing stroke. • Completed stroke (Stabilized). Dr. RS Mehta, BPKIHS
- 10. Infarct Stages: • Immediate – 6 hours – No Change both gross & microscopic • Acute stage – 2 days – Oedema, loss of grey/white matter border. – Inflammation • Intermediate stage – 2 Weeks – Demarcation – Liquifactive necrosis • Late stage – After Weeks – Fluid filled cysts with dark grey margin – Proliferation of glia, loss of architecture (Gliosis) . Dr. RS Mehta, BPKIHS
- 11. CVA • • • • Thromboetic infraction: 80% Cerebral Haemorrhage: 10% Sub-arrhochonoid hemorrhage: 5% Others Dr. RS Mehta, BPKIHS
- 12. Dr. RS Mehta, BPKIHS
- 13. Cerebral edema Dr. RS Mehta, BPKIHS
- 14. Local infarction: Dr. RS Mehta, BPKIHS
- 15. Dr. RS Mehta, BPKIHS
- 16. Cerebral Infarct - 1 Week Dr. RS Mehta, BPKIHS
- 17. Cerebral Infarct - 2 Weeks Dr. RS Mehta, BPKIHS
- 18. Cerebral Infarction - Late Dr. RS Mehta, BPKIHS
- 19. Dr. RS Mehta, BPKIHS
- 20. Causes: • • • Thrombosis. Embolus. Hemorrhage (HTN. Rupture). Dr. RS Mehta, BPKIHS
- 21. Risk factors • Modifiable risk factors – High BP – Cigarette smoking – Alcohol intake – Uncontrolled Heart disease – Atrial fibrillation – Uncontrolled Diabetes – Carotid congestion Dr. RS Mehta, BPKIHS
- 22. • • • • • High blood cholesterol Sedentary lifestyle Obesity Seasons Stress Dr. RS Mehta, BPKIHS
- 23. Risk Factors Unable to Control • • • • • • Age Gender Race Prior strokes Heredity Sickle Cell Disease Dr. RS Mehta, BPKIHS
- 24. Risk factors for stroke: • Non-modifiable: Age, Gender, Race, Prior CVA and Heredity. • Modifiable: HTN, DM, cardiac diseases, cigarette smoking, excessive Avenal intake, drug abuse, ↑ cholesterol. • Other factors: Obesity, migraines, oral contraceptives, hyper coagulation state. Dr. RS Mehta, BPKIHS
- 25. THREE STROKE TYPES Focal Brain Dysfunction Ischemic Stroke Intracerebral Hemorrhage 85% Clot occluding artery Subarachnoid Hemorrhage 10% Bleeding into brain 5% Bleeding around brain Diffuse Brain Dysfunction Dr. RS Mehta, BPKIHS
- 26. Pathophysiology Brain Very sensitive to loss of blood supply. Cannot resort anaerobic metabolism in the absence of oxygen and glucose. Hypoxia develop. Cerebral ischemia. Short term ischemia Temporary or TIAS Permanent infraction of cerebral cells. Dr. RS Mehta, BPKIHS (Permanent changes occur within 3-10 minutes).
- 27. Early warning signs: • Headache • Vomiting • Seizures • fever etc. Silent Stroke: do not cause Symptoms Dr. RS Mehta, BPKIHS
- 28. Signs and Symptoms of STROKE • Hemorrhagic – Sudden and dramatic – Violent explosive headache – Visual disturbance – Nausea and vomiting – Neck and back pain – Sensitivity to light – Weakness on one side Dr. RS Mehta, BPKIHS
- 29. Signs and Symptoms of STROKE • Ischemic Stroke – Harder to detect – Weakness in one side – Facial drooping – Numbness and tingling – Language disturbance – Visual disturbance Dr. RS Mehta, BPKIHS
- 30. Left Brain Damage • • • • Right side paralysis Speech and language disturbance Behavioral changes Swallowing problems Dr. RS Mehta, BPKIHS
- 31. Right Brain Damage • Left side paralysis • Coordination • Perception Dr. RS Mehta, BPKIHS
- 32. Specific deficits after CVA: • Hemiparesis and hemiplegia. • Apraxia (moves the part but not function properly). • Aphasia (difficulty in swallowing). • Visual changes: • Agnosia- recognition problem (object/person). • Incontinence. Dr. RS Mehta, BPKIHS
- 33. Clinical Manifestations • Affects many body functions • Motor activity • Elimination • Intellectual function • Perceptual alterations • Personality • Sensation • Communication Dr. RS Mehta, BPKIHS
- 34. Use a “FAST” STROKE Assessment • Face • Arm • Speech • Time of onset Dr. RS Mehta, BPKIHS
- 35. FACE • Look for Facial Droop – Have the patient smile or show his/her teeth – NORMAL Both sides of the face move equally – ABNORMAL One side of the patient’s face droops or does not move Dr. RS Mehta, BPKIHS
- 36. ARMS • Motor Weakness: Look for arm drift by asking the patient to close eyes and lift arms, palms up • NORMAL- arms remain extended equally or drift downward equally • ABNORMAL – One arm drifts down compared to the other Dr. RS Mehta, BPKIHS
- 37. SPEECH • Ask the patient to say “You can’t teach an old dog new tricks” • NORMAL –Phrase repeated clearly and plainly • ABNORMAL – Words slurred, abnormal or unable to speak Dr. RS Mehta, BPKIHS
- 38. Abnormal Speech • • • • Slurring of speech Unable to think of words Inappropriate words Expressive aphasia – unable to speak words • Receptive aphasia – unable to understand words Dr. RS Mehta, BPKIHS
- 39. TIME OF ONSET • The window of opportunity to effectively treat STROKE is 3 hours (180 minutes) – May be extended to 4 ½ hours • Need to know “ last known well”. • Difficult when – Patient lives alone – Woke up with symptoms Dr. RS Mehta, BPKIHS
- 40. Inv: • • • • X-ray skull, CT, MRI L.P. contra indicated if ↑ ICP ECG PET Scan: activities of brain and tissue damage • Angiography: visualize blood vessels Dr. RS Mehta, BPKIHS
- 41. Medical management: Aim: –Preserving life. –Minimizing residual deficits. –Reducing ICP. –Preventing extension or recurrence. Dr. RS Mehta, BPKIHS
- 42. Pharmacological management: • Anti coagulants, Anti-platelet therapy: (Heparin, Warfarin, Asprin, Tilcopidin). • Edema control: (steroid, osmotic diuretics (Mannitol) loop diuretics e.g. lasix). • Antihypertensive, mild analgesics: (avoid strong analgesic & sedative). • Seizure control: phenytoin / phenoharbitone. • Antibiotic (open HI). • Thrombolytic Agents (if blood Clot) Dr. RS Mehta, BPKIHS
- 43. Rx A. 1. CVA: Ischemic Tab. Asprin 150 mg, Po/NGT OD (Asprin allergy: Clopidogel 300mg stat,75mg/day) 2. Ranitidine/Ocid/Pantop: decrease gastric ulcer 3. Antihypertensive 4. O2 support: based on ABG, ABC 5. NGT feeding/IV infusion 6. Chest physiotherapy and passive exercise 7. DVT prophylaxis and Seizure control 8. Laxative 9. Catheter: Foleys early 10. Steroid: if Meningitis/ Inflammation / Swelling B. Clot: 11. anti-hypertensive 12. Mannitol-20% 13. Tissue Plasminogen Activator: t-PA (clot buster): previously STK was Dr. RS Mehta, BPKIHS used
- 44. tPA (Tissue Plasminogen Activator) – is a clot-busting drug – Ischemic strokes, the most common type of strokes, can be treated with a drug called t-PA, that dissolves blood clots obstructing blood flow to the brain. Dr. RS Mehta, BPKIHS
- 45. Surgical approaches: • Epidural (Clot): Excision & Drain • External ventrisculotomy drainage • Craniotomy: Flap of skull out- if cerebral decompression. • Extra / Intra-cranial bipass • Aneurysm: Clip • Internal Carotid Endarterectomy Dr. RS Mehta, BPKIHS
- 46. Dr. RS Mehta, BPKIHS
- 47. Dr. RS Mehta, BPKIHS
- 48. Internal Carotid Endarterectomy Dr. RS Mehta, > 70%) (if StenosisBPKIHS
- 49. Nursing Management Dr. RS Mehta, BPKIHS
- 50. Nursing management: Assessment • Initial assessment essential, includes: LOC, papillary reaction and movement of eye, changes in speech, sensory changes, reflexes, (planter: UMN / LMN), headache, and vital signs. • Recorded and scored in GCS (pupil movement response. / eye, motor, verbal). • Reports of: LP, CT, MRT etc. Dr. RS Mehta, BPKIHS
- 51. Nursing diagnosis: • Altered cerebral tissue perfusion R/T ↓ cerebral blood how (thrombus, embolus, hemorrhage, edema, spasm). Expected outcome: • The client will have improved cerebral tissue perfusion as evidenced by ICP less than 15 mm Hg, no report of headache and ↓ loc, stable, ↑ GCS score. Dr. RS Mehta, BPKIHS
- 52. Implementations: • Assessment of unstable client hourly. • Analyze data, if detorating inform physician. • Administer drug → asprin, heparin, tilcopidine. • Delirium or restlessness should be controlled with sedatives, if necessary. (Be sure restlessness is not due to: hypoxia, full bladder, bowel impaction, pain etc). • Restraints should be avoided, became they often increase agitation and ↑ ICP. Dr. RS Mehta, BPKIHS
- 53. • Straining at stool, or with excessive coughing, vomiting, lifting of the arms to change position should be avoided. (↑ ICO). • Mild laxatives and stool softeners are often prescribed. • The client who is a wade and alert should be taught about the pathologic process and instructed to inform you about any changes in: Sensation, movement, or function, regardless of how minor a change may seem. Dr. RS Mehta, BPKIHS
- 54. • Impaired physical mobility R/T loss of muscle tone secondary to flaccid paralysis or spasticity or reluctance to move associated with fear of self – injury or prolong disuse. Dr. RS Mehta, BPKIHS
- 55. Risk for impaired skin integrity R/T loss of protective sensation and decreased ability to move. • Expected Outcome: The client’s skin will remain intact as evidenced by no stage I pressure ulcer development and no signs of redness from friction or shearing. Dr. RS Mehta, BPKIHS
- 56. Risk for contracture R/T flaccid paralysis or spasticity. • Expected Outcome: The client will have absence of contractures joint, ankylosis, muscle shortening as evidenced by maintaining normal Rom. Dr. RS Mehta, BPKIHS
- 57. Impaired verbal communication R/T loss of the function of muscle, which produces speech or ischemia of the dominant cerebral hemisphere. • Expected Outcome: The client will be able to effectively communication. Dr. RS Mehta, BPKIHS
- 58. Ineffective individual coping RT physiologic changes and frustrations. • Expected Outcome: The client will develop effective coping strategies, as evidenced by appropriate life-style modifications, use of the assistance of others, and appropriate social interactions. Dr. RS Mehta, BPKIHS
- 59. Long term care of stroke patient (Rehabilitation): Aims: • To prevent further impairment. • Jo maintain existing abilities and • To restore highest level of function possible. – TRF → bed to wheel chair. (Hemiplegia). – Assess daily living activities (ADL => score (0-100). • => Bowel, bladder, grooming, toilet use, transfer, mobility, dressing, stairs, bathing. (0, 5, 10) => evaluate prognosis. – Glasgow coma scale: Eye open (4), Verbal (5), Moter (6). Dr. RS Mehta, BPKIHS
- 60. Nursing care of the Patient undergoing intracranial surgery: • • • • Potential for ineffective breathing pattern RT post operative cerebral edema. Potential for alteration in fluid volume RT ↑ ICP or dieresis. Alteration in sensory perception RT periorbital edema and head dressing. Monitor and manage complication: Cerebral edema, intracranial hemorrhage, seizures, infection, venous thrombosis, leakage of CSF, (G.I. ulceration: monitor S/S of hemorrhage, perforation or both). Dr. RS Mehta, BPKIHS
- 61. Short and long term effects • The physical damage stroke causes to the brain can have a wide range of effects that will depend on the type of stroke and its severity, the part of the brain affected the extent of brain damage and how quickly other brain cells take over the function of those that are damaged or dead. Around a third of strokes are fatal. • Effects may include: next page Dr. RS Mehta, BPKIHS
- 62. Effects • • • • • • • • • • • • Weakness or paralysis Lack of feeling Swallowing difficulties Speech or language difficulties Problems of perception Cognitive difficulties Behaviour changes Difficulties with bowel or bladder control Fatigue Mood changes Post-stroke pain Epilepsy: (7-20%) Mehta, BPKIHS Dr. RS
- 63. Rehabilitation: (Nurses role) • Exercise. • Diet. • Regular follow up. • Family support. • Psychological support. • Occupational therapy. Dr. RS Mehta, BPKIHS
- 64. Nursing Care of Bed Ridden Patients ( Summary) 1.Regular change of position. 2.Care of skin and pressure sore, 3.Bladder management. 4.Care of bowel. 5.Management of diet. 6.Chest physiotherapy. 7.Rehabilitation & physiotherapy. 8.Recreational and Divertional therapy. 9.Occupational therapy. Dr. RS Mehta, BPKIHS
- 65. Primary Prevention: Decrease Risk Factors 1. Treatment of HTN 2. Avoid Smoking 3. Active Life Style 4. Avoid Alcohol 5. Decrease LDL Cholesterol 6. Anticoagulant in Atrial Fibrillation Dr. RS Mehta, BPKIHS
- 66. Dr. RS Mehta, BPKIHS
- 67. Dr. RS Mehta, BPKIHS
- 68. Thank you Dr. RS Mehta, BPKIHS