

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a 23204910
Semelhante a 23204910 (20)
Mais de radgirl
Último
Último (20)
23204910
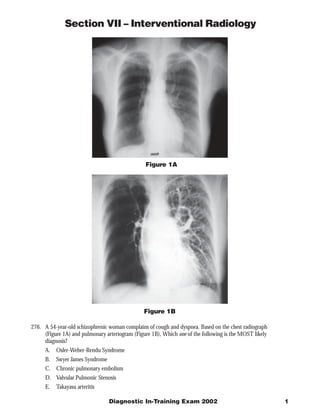
- 1. Section VII – Interventional Radiology Figure 1A Figure 1B 276. A 54-year-old schizophrenic woman complains of cough and dyspnea. Based on the chest radiograph (Figure 1A) and pulmonary arteriogram (Figure 1B), Which one of the following is the MOST likely diagnosis? A. Osler-Weber-Rendu Syndrome B. Swyer James Syndrome C. Chronic pulmonary embolism D. Valvular Pulmonic Stenosis E. Takayasu arteritis Diagnostic In-Training Exam 2002 1
- 2. Section VII – Interventional Radiology Question #276 Findings: The chest radiograph demonstrates a normal sized heart and normal left hemithorax, including pulmonary vasculature. The angiogram confirms a small right pulmonary artery. The right main pulmonary artery is small and the right lung is hyperlucent due to a diffuse decrease in pulmonary vascularity. Rationales: A) Incorrect. Osler-Weber-Rendu Syndrome, also known as hereditary hemorrhagic telangiectasia, is an autosomal dominant disorder resulting in diffuse vascular dysplasia. The dysplasia is manifested as arteriovenous malformations (small ones are called telangiectasias), and aneurysms. Pulmonary arteriovenous malformations occur in 5-15% of patients. This disease does not result in diffuse hypoplasia of a vascular bed. B) Correct. Swyer James Syndrome is the result of acute viral bronchiolitis in infancy or early childhood that prevents further normal lung development. Symptoms include cough, dyspnea on exertion, hemoptysis, and recurrent lower respiratory infections. Radiographic abnormalities may be present even in asymptomatic individuals. Pathologic findings include a small hemithorax, diffuse bronchiectasis, emphysematous changes in the lung parenchyma, and a diffusely small pulmonary arterial tree. The findings usually involve one lung, but may be restricted to a single lobe, or involve both lungs. Ventilation perfusion scanning demonstrates air trapping and diffusely decreased perfusion in the affected region. Bronchiectasis is evident on high resolution CT. The pulmonary arterial tree is intrinsically normal but is small because it subserves a decreased amount of lung parenchyma. C) Incorrect. Chronic pulmonary embolism can cause the pulmonary arteries to be small and the arterial tree to have a pruned appearance. Chronic PE, however, does not affect a single lung; abnormalities will be evident in both lungs. In addition, the arteries are intrinsically abnormal; findings include abrupt occlusion of vessels, irregularity of the vessel wall, and intravascular webs. These abnormalities are the result of clot retraction and fibrosis. Finally, in chronic PE, the central pulmonary arteries can be quite large due to the pulmonary arterial outflow obstruction. D) Incorrect. Isolated valvular pulmonic stenosis is one of the most common congenital heart diseases diagnosed in adulthood. It may require no treatment or may lead to clinically significant right ventricular outflow obstruction. The most common presenting symptoms are due to exercise intolerance, and may include fatigue, dyspnea, chest pain and syncope. Pathologic findings resulting from the narrowed valve orifice include right ventricular hypertrophy and post stenotic dilation of the main pulmonary artery. Because of the direction of the jet effect, the left pulmonary artery may also be dilated. The right pulmonary artery and peripheral arterial tree are usually normal. In this case, there is no evidence of right ventricular hypertrophy or enlargement of the main pulmonary artery on the chest radiograph. In addition, the right pulmonary arterial tree is clearly hypoplastic. E) Incorrect. Takayasu arteritis is a granulomatous inflammation affecting the aorta, its major branches, and the pulmonary arteries. It is of unknown etiology and usually presents in patients younger than age 50. Radiographic findings include systemic arterial stenosis and occlusions, although regions of vascular dilation can occur. The pulmonary arteries may be involved. Pulmonary arterial abnormalities include multiple segmental stenoses and occlusions that mimic chronic pulmonary embolism. Because of the diffuse nature of the disease, both lungs are typically. Due to outflow obstruction, the central pulmonary arteries may be enlarged. As is seen in the systemic circulation, affected pulmonary arteries are thick-walled on cross-sectional imaging. 2 American College of Radiology
- 3. Section VII – Interventional Radiology Figure 2A Figure 2B Figure 2C 277. A 29-year-old woman with a history of IV drug abuse presents with spiking fevers and bilateral lower extrem- ity pain. On physical examination, she has a heart murmur as well as decreased lower extremity pulses. Based on two images from an abdominal aortogram (Figures 2A and 2B), and one image from a pelvic arteriogram (Figure 2C), which one of the following is the MOST likely diagnosis? A. Atherosclerosis B. Embolus C. Dissection D. Coarctation E. Trans-section Diagnostic In-Training Exam 2002 3
- 4. Section VII – Interventional Radiology Question #277 Findings: The abdominal aorta and its major visceral branches are normal. There is a large filling defect at the aortic bifurcation extending across the origins of both common iliac arteries. The iliac arteries beyond their origins are normal. Rationales: A) Incorrect. Except for the filling at the aortic bifurcation, the arteries here are normal. They have smooth margins, they are of normal caliber, and they taper gradually as they course peripherally. The iliac arteries are diffusely small, but this can be explained by the obstruction to inflow by the large filling defect at the aortic bifurcation. Atherosclerotic changes include vessel wall calcifications, marginal irregularity of vessels, and segmental stenosis that may be concentric or eccentric. The aortic bifurcation is a common site for atherosclerotic stenosis or occlusion to occur – especially in elderly smokers. However, it would not against in a background of otherwise normal vessels. Other vessels would demonstrate changes of atherosclerosis. In addition, atherosclerotic occlusions occur gradually, allowing collateral vessels to develop. Collaterals that result from atherosclerotic occlusion of the distal aorta typically arise from lumbar arteries. The lumbar arteries here are of normal caliber and course. B. Correct. This is a classic appearance of an embolus: a filling defect with menisci at its borders with patent lumen. In addition, emboli typically lodge at bifurcation points, as is the case here. Other vessels are normal. The patient’s history in this case suggest that the source of the embolus may be bacterial endocarditis. C. Incorrect. A dissection occurs when a partial thickness tear occurs in the arterial wall, allowing blood to flow within a channel that develops in the medial layer. The classic arteriographic finding is a liner filling defect within the artery that spirals along the course of the artery. Re-entry tears occur at branch points. The false channel can thrombose; when that happens the arteriogram demonstrates smooth narrowing of the residual true lumen. An abrupt short occlusion with menisci is not characteristic of a dissection. D. Incorrect. Coarctation is a congenital narrowing or occlusion of the aorta. Coarctation of the thoracic aorta typically presents in childhood. Congenital abdominal aortic coarctation is rare, and may present in young adults. Its etiology is poorly understood; it may be the result of incomplete fusion of the two embryonic dorsal aortas. Congenital abdominal aortic coarctation appears as a smooth tapered narrowing of the vessel. It may involve the origins of one or more visceral vessels. Coarctation at or above the level of the renal arteries usually presents with hypertension.. Coarctation of the infrarenal aorta may present with claudication. Large collateral channels are invariably present. With infrarenal coarctation, collateral supply to the legs arises from the lumbar and inferior mesenteric arteries, and possibly the internal mammary arteries. E. Incorrect. A trans-section is a circumferential laceration of the vessel wall. Aortic trans-section is invariably the result trauma, typically deceleration injury. Aortic trans-section usually occurs as a result of high speed motor vehicle accident. The common locations for this injury are the aortic root, the aortic isthmus, and the aorta at the level of the diaphragm. Of these, root injuries are the most common in autopsy series; isthmus injuries are most common among patients who live long enough to reach medical care. Abdominal aortic trans-section is relatively rare but may occur. In small peripheral arteries, trans-section may result in arterial occlusion at the site of injury. This is not the case in the large caliber, high flow aorta. With aortic trans-section, the classic angiographic finding is extravasation of contrast from the vessel lumen into an irregular but contained vascular space commonly called a pseudoaneurysm. The pseudoaneurysm is contained by the connective tissue surrounding the aorta. Free extravasation of contrast is rare and when it occurs is a premorbid event. 4 American College of Radiology
- 5. Section VII – Interventional Radiology Figure 3 278. A 37-year-old man underwent arteriography because of upper GI hemorrhage unresponsive to endoscopic therapy. Which one of the following is the name of the labeled artery? (Figure 3) A. Right gastric artery B. Dorsal pancreatic artery C. Inferior pancreatico-duodenal artery D. Gastro-epiploic artery E. Middle colic artery Diagnostic In-Training Exam 2002 5
- 6. Section VII – Interventional Radiology Question #278 Findings: This is a normal celiac arteriogram. The labeled artery is the gastro-epiploic artery, the terminal branch of the gastro-duodenal artery. It courses along the greater curvature of the stomach. The major branches of the celiac axis are the splenic, left gastric and common hepatic arteries. In about 50% of people, including this patient, the inferior phrenic arteries also arise from the celiac axis. This patient’s hepatic arterial supply is non-standard: the left hepatic artery arises from the left gastric artery, this occurs in about 25% of patients. Rationales: A) Incorrect. The right gastric artery is a small vessel that is frequently not seen on celiac arteriography. It usually arises from the proper hepatic artery or the proximal left hepatic artery. It courses along the lesser curvature of the stomach to anastomose with terminal branches of the left gastric artery. B) Incorrect. The dorsal pancreatic artery is a large short vessel that courses vertically from the celiac axis or splenic artery to provide blood supply to the body of the pancreas. It gives off the transverse pancreatic artery which courses along the long axis of the pancreas. It also anastomoses with branches of the pancreatico-duodenal arcade. Although its origin can be variable, it does not arise from the gastroduodenal artery and does not have the long course demonstrated by the gastroepiploic artery. C) Incorrect. The inferior pancreatico-duodenal artery arises from the proximal superior mesenteric artery (SMA) or from a jejunal branch of SMA. It branches into anterior and posterior divisions that wrap around the head of the pancreas to anastomose with the superior pancreatico-duodenal branches of the gastroduodenal artery. You can fill this vessel on a celiac arteriogram but you would expect to see contrast reflux from it into SMA. D) Correct. The labeled artery is the gastroepiploic artery. This terminal branch of the gastroduodenal artery runs along the greater curvature of the stomach, supplying branches to the stomach as well as to the omentum. The gastroduodenal artery is one of two major branches of the common hepatic artery. The other is the proper hepatic artery. The arteries can be named correctly by assessing where they arise and where they travel. E) Incorrect. The middle colic artery arises from the proximal superior mesenteric artery and has a typical branching pattern. It branches in a “T”-like fashion into right and left branches which course along the mesenteric border of the transverse colon. Rarely, this vessel can arise from the celiac axis or from the dorsal pancreatic artery. It does not arise from the gastroduodenal artery. 6 American College of Radiology
- 7. Section VII – Interventional Radiology Figure 4 279. A 54-year-old woman with a history of cirrhosis, chronic pancreatitis and recurrent GI hemorrhage presented with lower GI bleeding. Visceral arteriography was performed. Based on this film from the venous phase of a superior mesenteric arteriogram (Figure 4), which one of the following is the MOST likely diagnosis? A. Arteriovenous malformation B. Pancreatic cancer C. Chronic portal vein occlusion D. Budd Chiari Syndrome E. Spontaneous spleno-renal shunt Diagnostic In-Training Exam 2002 7
- 8. Section VII – Interventional Radiology Question #279 Findings: There is dense opacification of veins throughout the mesentery. In the periphery of the mesentery, the veins have a normal course and location. In the region of the root of the mesentery, there is a tangle of varicosities which course along the expected location of the main superior mesenteric vein and main portal vein. In the right upper quadrant, the varicosities drain into a vein that could be mistaken for the main portal vein. However, it is small and irregular; it terminates in a tangle of small vessels in the liver hilum. Normal intrahepatic portal vein branches can be seen in the periphery of the liver. The splenic vein is not seen. Rationale: A) Incorrect. An arteriovenous malformation in the superior mesenteric circulation could cause dense venous opacification. It could also be the source of recurrent GI hemorrhage. It could cause varicosities to develop due to high flow. However, you would expect to see simultaneous opacification of arteries and veins. An AVM would not lead to portal vein occlusion. Therefore, you would expect to see varices in addition to a large portal vein. B) Incorrect. Pancreatic cancer can cause encasement, invasion, compression, and occlusion of the superior mesenteric and portal veins. However, because pancreatic cancer is typically an aggressive disease, these changes occur relatively rapidly. Varicosities do not develop, presumably due to concurrent invasion of potential collateral channels and because of lack of time prior to the patient’s death. C. Correct. The superior mesenteric, and portal veins do not fill on this superior mesenteric arteriogram. Large varicosities replace them. This is the classic appearance of “cavernous transformation of the portal vein”, or chronic portal venous occlusion. In this case the central right and left portal vein branches are involved as is the superior mesenteric vein. The central venous occlusion is most likely the result of chronic pancreatitis. The splenic vein is also probably occluded, at least centrally. The varicosities arise from small periportal and peribiliary veins that dilate over time. Chronic portal vein occlusion can occur following sepsis or pancreatitis, or as a result of cirrhosis. It can occur in infants after umbilical vein catheterization. D. Incorrect. Budd-Chiari syndrome is the result of obstruction to hepatic venous outflow – due either to thrombosis of peripheral intrahepatic vein branches; central hepatic vein webs, or IVC obstruction. There is no association with pancreatitis. The portal system is normal, although the portal pressures are high and flow in the portal vein may be reversed. E. Incorrect. A spontaneous spleno-renal shunt occurs as a natural decompression pathway in patients with portal hypertension and a patent splenic vein. The angiographic appearance includes filling, from the splenic vein, of a large cluster of varicosities in the left upper quadrant of the abdomen that drains caudally into the inferior vena cava via the left renal vein. This arteriogram demonstrates none of the findings of spleno-renal shunt. 8 American College of Radiology
- 9. Section VII – Interventional Radiology Figure 5A Figure 5B 280. A 17-year-old male is referred for angiography because of severe hypertension. His erythrocyte sedimentation rate is normal. Based on two films from an aortogram (Figures 5A and 5B), which one of the following is the MOST likely diagnosis? A. Atherosclerosis B. Medial fibroplasia C. Poly arteritis nodosa D. Granulomatous arteritis E. Neurofibromatosis Diagnostic In-Training Exam 2002 9
- 10. Section VII – Interventional Radiology Question #280 Findings: The films demonstrate that the aorta is normal – straight and smooth. There are high-grade orificial stenoses of both the right and the left renal arteries. The main renal arteries and renal artery branches are otherwise normal. Rationales: A) Incorrect. This patient is too young to have atherosclerosis this advanced. In addition, the aorta and peripheral renal arteries are normal. Hemodynamically-significant atherosclerotic stenosis does not occur against a background of completely normal vessels. If you look, you will always see further evidence of arterial disease – such as irregular walls, mild stenosis, and pruning of peripheral branches. B) Incorrect. Medial fibroplasia is the most common type of fibromuscular dysplasia. It typically occurs in the mid renal arteries sparing the vessel origins in almost all cases. The classic angiographic appearance is a “string of beads”, with multiple webs alternating with short areas of vessel dilatation. The abnormality in this angiogram doesn’t look like medial fibroplasia. C. Incorrect. Polyarteritis Nodosa is a systemic necrotizing inflammation of medium-sized and small muscular arteries. The disease is typically associated with fever, arthralgias, myalgias, and an elevated sedimentation rate. It is more common in men than in women. The primary angiographic manifestation of the disease is demonstration of multiple small saccular aneurysms of medium and small arterial branches. The renal arteries are most commonly involved. Branch arterial stenosis and occlusions can also occur. Isolated stenosis of the main renal artery does not occur. D. Incorrect. Granulomatous arteritis is an infiltrative granulomatous process in the arterial wall that can progress to fibrosis and vessel occlusion. It is typically associated with a flu-like prodrome, and is invariably associated with an elevated erythrocyte sedimentation rate. It is morphologically indistinguishable from Takayasu arteritis. It occurs typically in adults over age 50, peaking at ages 65 – 75. It causes long segment stenosis and occlusions. The classic site of involvement is the temporal artery. E. Correct. Orificial renal artery stenosis is a classic finding in patients with neurofibromatosis and hypertension. The renal artery involvement is typically found in childhood due to the associated hypertension. The stenosis may be due to either dysplasia of the arterial wall itself (most common), or due to narrowing of the vessel by a periarterial neurofibroma (rare). The primary differential diagnostic possibility in this case is congenital renal artery stenosis. Renal artery stenosis due to neurofibromatosis can narrow the renal arteries a bit more peripherally than is seen in this case. When that happens, the differential diagnosis must also include the smooth forms of fibromuscular disease (such as intimal fibroplasia). 10 American College of Radiology