4.11 Amanda Andere: Homeless Assistance Referral Form
•
1 gostou•1,122 visualizações


Recomendados
Recomendados
Mais conteúdo relacionado
Destaque
Mais de National Alliance to End Homelessness
Mais de National Alliance to End Homelessness (20)
4.11 Amanda Andere: Homeless Assistance Referral Form
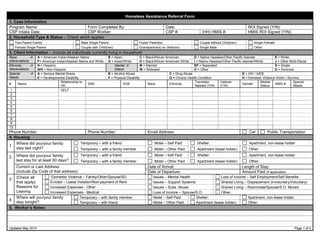
- 1. Homeless Assistance Referral Form 1. Case Information Program Name: Form Completed By: Date: ROI Signed (Y/N): CSP Intake Date: CSP Worker: CSP #: (HH) HMIS #: HMIS ROI Signed (Y/N): 2. Household Type & Status – Check which applies Two-Parent Family Male Single Parent Foster Parent(s) Couple without Child(ren) Single Female Female Single Parent Couple with Child(ren) Grandparent(s) w/ child(ren) Single Male Other: 3. Client Information – Include all individuals currently living in household Race A = American Indian/Alaskan Native B = Asian C = Black/African American D = Native Hawaiian/Other Pacific Islander E = White Abbreviations F= American Indian/Alaskan Native and White G = Asian/White H = Black/African American/ White I = Native Hawaiian/Other Pacific Islander/White J = Other Multi-Racial Ethnicity H = Hispanic Marital M = Married SP = Separated S = Single Abbreviations N/H = Non-Hispanic Status W = Widowed O = Other D = Divorced Special A = Serious Mental Illness B = Alcohol Abuse C = Drug Abuse D = HIV / AIDS Needs E = Developmental Disability F = Physical Disability G = Chronic Health Condition H = Domestic Violence Victim / Survivor Relationship to Translator Veteran Marital Special # Name SSN DOB Race Ethnicity Gender HMIS # HH Needed (Y/N) (Y/N) Status Needs 1 SELF 2 3 4 5 6 7 8 9 10 Phone Number: Phone Number: Email Address: Car Public Transportation 4. Housing Where did you/your family Temporary – with a friend Motel – Self Paid Shelter: Apartment, non-lease holder 1 stay last night? Temporary – with a family member Motel – Other Paid Apartment (lease holder) Other: Where did you/your family Temporary – with a friend Motel – Self Paid Shelter: Apartment, non-lease holder 2 last stay for at least 90 days? Temporary – with a family member Motel – Other Paid Apartment (lease holder) Other: Current or Last Address Date of Arrival: Length of Stay: (Include Zip Code of that address): Date of Departure: Amount Paid (if applicable): *Domestic Violence – Family/Other/Spouse/SO Issues – Mental Health Loss of Income – Self Employment/Self Benefits 3 (Check all that apply): Evicted – Lease Violation/Non-payment of Rent Issues – Support Systems Shared Living – Displacement (Involuntary/Voluntary) Reasons for Increased Expenses - Other Issues – Subs. Abuse Shared Living – Roommate/Spouse/S.O. Moved Leaving Increased Expenses - Medical Loss of Income – Spouse/S.O. Other: Where will you/your family Temporary – with family member Motel – Self Paid Shelter: Apartment, non-lease holder 4 stay tonight? Temporary – with friend Motel – Other Paid Apartment (lease holder) Other: 5. Worker’s Notes: Updated May 2010 Page 1 of 2
- 2. 6. Income (during last 30 days) – Write in the amount or write “X” if the CL is not receiving. Type / Cash Amount Type / Cash Amount Type / Cash Amount Type / Non-Cash Amount Employment Unemployment Court Awards View/FSET TANF Workman’s Comp Pension/401k Food Stamps General Relief SSI Tax Refund Housing Subsidy/Choice Child Support Social Security Other: Other: Alimony SSDI Other: Other: TOTAL AMOUNT OF GROSS INCOME (Do not include Non-Cash Benefits) 7. Financial Resources – For “Other Account,” include pension, 401k, IRAs, VIDA Checking Account (Balance, Bank Name): Savings Account (Balance, Bank Name): Other Account (Balance, Bank Name): Other Account (Balance, Bank Name): 8. Expenses (30 days) – Write in the amount or write “X” if the CL does not have the expense. Type Amount Type Amount Type Amount Type Amount Rent/Mortgage Utilities Work/School exp Prescriptions/Other Car Insurance Cable/Internet/Bundle Fines/Fees Alimony Car Payment Child Support Credit Card Payments Child Care Gas/Maintenance Groceries TANF/Government Health Ins./Co-Pay Bus Fare/Parking Telephone/Cell Phone Taxes/Registration Other: TOTAL AMOUNT OF EXPENSES: 9. Employment Information – Check “N/A” if no one in the household is employed and skip to Section 10 Name of Person Employed: Current Employer: Phone: N/A Hourly Wage: FT or PT: Benefits (Y/N): Hours per week: Start Date: End Date: Name of Person Employed: Current Employer: Phone: N/A Hourly Wage: FT or PT: Benefits (Y/N): Hours per week: Start Date: End Date: Name of Person Employed: Current Employer: Phone: N/A Hourly Wage: FT or PT: Benefits (Y/N): Hours per week: Start Date: End Date: 10. Triage Assessment – Answer the following questions to assess the appropriate referral for the client. Worker’s # Y N N/A Questions # Y N N/A Questions Worker’s Notes/Answer Notes/Answer Do you have a lease currently in your Do you have savings? If yes, how 1 5 name? much: If you have been evicted for something other 2 than non-payment of rent, list reason: Do you have friends or family that 6 you can live with? If yes, list any Are your rent/mortgage and utilities paid 3 possible stipulations: up to date? If no, amount owed: Do you need assistance securing Do you have a pay or quit notice or 7 4 housing? If yes, list requested summons for court? If yes, list date: assistance: Prevention, Diversion, or Shelter – Complete the following assessment to determine which area best describes the CL. Refer for Prevention if all of the following apply Refer for Diversion if all of the following apply. Refer for Shelter if all of the following apply. CL is currently in a living environment that can be CL has no place meant for human habitation to sleep CL cannot be maintained in their current living situation. maintained with financial assistance. tonight. CL’s living arrangement meets regulations regarding number of people who can reside in the residence. CL has a safe place to sleep temporarily while other CL has no identified support system that can provide CL is paying less than 50% of their income towards living arrangements can be made. housing temporarily. household expenses i.e. rent, utilities. Referred to (Agency Name): Referred to (Agency Name): Referred to (Agency Name): Updated May 2010 Page 2 of 2