

Recomendados
Recomendados
Mais conteúdo relacionado
Semelhante a 3.2 Michelle Heritage 1
Semelhante a 3.2 Michelle Heritage 1 (20)
Mais de National Alliance to End Homelessness
Mais de National Alliance to End Homelessness (20)
3.2 Michelle Heritage 1
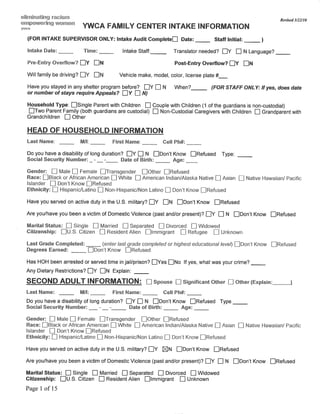
- 16. YWCA Family Center Triage Form Revision effective 08-07-09 Staff name: ____________________ Date: ___/___/___ Time: _____AM/PM Phone Call Walk-In In order to determine your eligibility for our program, the YWCA Family Center needs to collect data and information about you and your household. This information collected, both on paper and electronically, is considered confidential and privileged and the YWCA will only use this information for planning purposes, in conjunction with its funder, the Community Shelter Board. Are you willing to provide this information? Yes No 1. What is your name (Confirm Spelling?) _________________________ Any other name(s):_____________________ DOB:___/___/____ Gender:_____ SS#:_______/______/_______ Race: Black White Native American Asian Hispanic Employed: Yes No Other adult in household(Confirm Spelling?) _________________________ Any other name(s):_____________________ DOB: ___/___/____ Gender:_____ SS#:_______/______/______ Race: Black White Native American Asian Hispanic Employed: Yes No 2. Do you have minor children with you now? Yes No If so, do you have legal custody of them? Yes No How many children? _______ Ages? ______0-2 years ______ 3-7 years ______ 8-12 years ______ 13-17 A. If the answer is yes to both, proceed to next question. B. If the caller does not have minor children please refer to an appropriate single system provider and record referral C. .If the caller does not have legal custody of their children please explain our policy and offer appropriate resources and record referral 3. Where are you calling from?____________ Is there a phone number there?____________ Alternate contact #:___________ 4. Last address where you had housing in your name?_______________________________ Zip Code:_________ When?____ 5. What is the situation there? ________________________________________________________________________________ ___________________________________________________________________________________________________________ ___________________________________________________________________________________________________________ - If facing eviction, ask “Have you received an eviction notice?” Yes No - If Yes when is the court date? ____________ - If a landlord or other legal problem, ask “Have you contacted Legal Aid?” Yes No - If a utilities problem, ask “Have you talked to the utility company?” Yes No - If housing is condemned, ask “Have you contacted the City/County for assistance? “ Yes No 6. Where did you stay last night? __________________________________________________________ Zip Code:__________ 7. Is that in Franklin County? Yes No If no, where?: ____________________________ A. If the caller was a resident of Franklin County prior to becoming homeless, proceed to next question. B. If the caller is from out of county, ask “What is your housing plan for Franklin County?” _____________________________________________________________________________ C. If the caller has no feasible plan, state: “The YWCA Family Center provides temporary shelter and/or services to families who were living in Franklin County prior to becoming homeless. Do you have housing or resources in ____________________ (county where last housing was)? Yes No - If yes, assist family with accessing resources in their community. If necessary, you may seek approval from a YFC director to authorize an overnight courtesy stay while we assist them. If no, proceed to next question. 8. Have you ever been in a shelter program before? Yes No What program? _______________ When:___________ A. If no, please verify in CSP and move to next section. Does CSP show past stays? Yes No, if Yes proceed to B B. If yes, please verify in CSP and record date of all previous entries: ______________________________________ Outcome of last shelter stay:_____________________________________________________________________ 9. Are you or anyone one in your household a registered sex offender? Yes No A. If no, move to next section. B. If yes, family isn’t eligible for our program, explain our policy and offer appropriate resources and record referral 10. Are you safe right now? Yes No If no, why? ________________________________________________________________________________________________ If the caller is safe right now, proceed to next question. A. If the caller is not safe due to domestic violence, assess immediate risk and make appropriate referrals and record. B. If the caller is not safe due to some other condition, make appropriate referral and record. 11. Is there anyone else you and your family could stay with for at least the next two business days so that it may be determined if you are eligible for other services and/or supports that may prevent your entry into emergency shelter: Yes No 12. Has anyone in your home including adults ever been involved in Child Protective Service: Yes No if yes, who:_______ A. If the answer is no, proceed to next section B. If the answer is yes, determine eligibility for Stable Families (if caller expresses support but not able to get there please problem-solve transportation with family as needed) and make appropriate referrals and record. Cab Voucher provided: Yes No
- 17. Stable Families: Staff: Did the family answer yes to questions 10 and 11or was the family’s most recent permanent address or their current address located in one of the following zip codes: 43203, 05, 06, 13, 20? If the family meets either of these qualifiers and can remain where they are and prevent their need to enter shelter for at least the next two business days they are an appropriate referral. If the family is willing to participate in a screening to determine eligibility proceed with the following request for consent: “We are an agency partner of the Community Shelter Board who is sponsoring a prevention program, Stable Families, for families in Franklin County experiencing a housing crisis. If you would like the YWCA Family Center to refer your family to this program so that someone will contact you to determine eligibility for case management and limited financial support we will need your verbal consent? Do you give the YWCA Family Center your consent to refer your family to the Stable Families program? Yes No If yes, contact Stable Families by e-mail and/or phone and fax a copy of the Triage form, if no, proceed with Eligibility and Outcome Referral Type: Referral Source and Contact: Referral Made: Prevention Pilot – CSB Stable Families – 268-2472 ext. 22 Fax 268-4260 Yes No Julie Holston (e-mail; jholston@ciskids.org) Shelter for Single Men Faith Mission – 224-6617 Yes No Faith on 8th - 299-3192 Yes No Friends of the Homeless (FOH) – 253-2770 Yes No Volunteers of America – 224-0128 Yes No Shelter for Single Women Nancy’s Place (Faith Mission) – 224-6617 Yes No Rebecca’s Place (FOH) – 253-2770 Out of County Firstlink – 221-2255 or 211 Yes No Domestic Violence – (Single women and women CHOICES – 224-4663 Yes No w/children) Alcohol / Drug Treatment Amethyst - Yes No Maryhaven Engagement Center – 449-1530 (Men) 324-5413 (Women) Mental Health Services Netcare – 276-2273 Yes No Rental Assistance Homeless Prevention Program – Gladden Community House – Yes No 2217801 Donna Woods Landlord Mediation and Resolution Legal Aid – 241-2003 Yes No Utility Assistance HEAP 800-686-1557 Yes No Please list other resources provided: ____________________________________________________________ Eligibility and Outcome If the caller meets eligibility for entry into the program and has no other options, please provide a brief description of our program model, rules, and expectations, and schedule an Intake. 1) YFC is a temporary emergency shelter program for families in housing crisis. 2) Target stay is 14-21 days. 3) The family will be required to meet with an assigned Family Advocate at least 2-3 times per week, and create and follow through on their housing goal plan, including securing next step housing. 4) The YFC is an alcohol and drug free facility. 5) Curfew is 6:00 every night unless you have verifiable employment. 12. Eligibility Determination (Please attach additional documentation, case notes, or incident reports as necessary.) A. Does caller meet eligibility for entry into the program? Yes No B. If no, why not? ________________ If Applicable was family informed of their right to Appeal this decision: Yes No C. Was family scheduled for Appeals? Yes No If yes, when? Date: ________ Time: _____ Re-Entry Yes No Self requested due to ineligibility Yes No D. Was family scheduled for Intake? Yes No If yes, when? Date: ________ Time: _____ Notes:_________________________________________________________________________________________________________ ___________________________________________________________________________________________________________ Office use: Did family enter program? Yes No If yes, date family entered: _________ Staff name: (print) __________________________________ Staff signature: ___________________ This data has been entered into CSP Yes No Staff Initials: ________ 2
- 19. Faith Mission/Faith Mission Triage Form Name of Individual Requesting Shelter SSN TRIAGE: Welcome to Faith Mission. My name is (STATE YOUR NAME). I will be working with you today as we explore whether Faith Mission's Emergency Shelter program is the best place for you at this point in time. Please understand that emergency shelter is only an option for you when there is no other place where you can stay. Also, the demand for a program bed is very high right now and we cannot guarantee a place for you in our program. Triage Performed By: _______________________________________ Date:_______________________________ Type of Triage: ___Walk-In ____Telephone Time:_______________________________ IF A TELEPHONE TRIAGE PLEASE PROCEED TO TELEPHONE TRIAGE DIVERSION SCRIPT IF A WALK-IN TRIAGE PROCEED TO A A) Are you looking to obtain services for tonight? ____ Yes ____No IF YES, PROCEED TO B IF NO, PROCEED TO TRIAGE SCRIPT BELOW TRIAGE: Demand for a shelter bed is very high and we cannot reserve a space for you in our program unless you are ready to enter the program immediately. We perform triage and intake services 24 hours a day. If you are in need of shelter, please call us or visit our Intake Center at 315 E. Long Street or visit a shelter site if the Intake Center is closed. In the mean time, if you are in danger of becoming homeless, I would like to suggest that you contact one of the following agencies to request assistance in maintaining your current housing. Do you have a pen and a piece of paper? Okay, here are the telephone numbers: First Link 211; CCCS of the Midwest (800) 355-2257; Columbus Housing Partnership, Inc. (614) 221-8889; Columbus Urban League (614) 257-6300. Thank you for calling. PROCEED TO THE DISPOSITION SECTION ON THE FINAL PAGE OF THIS FORM, SELECT DISPOSITION 2 B) Is there a telephone number where you can be reached? __________________________________________ C) (TELEPHONE ONLY) Can you tell me the address and/or location you are currently calling from? _________________________________________________________________________________________________ D) Is the individual under a service restriction? _____Yes _____No IF NO, PROCEED TO QUESTION 1 IF YES, PLEASE USE TRIAGE SCRIPT BELOW TRIAGE: Our records show that you are currently under a service restriction with Faith Mission and are not eligible for shelter. If you would like to dispute this current restriction I can provide you with an appeals package and have your concern heard by the appeals committee according to our shelter appeals procedure. PROCEED TO THE DISPOSITION SECTION ON THE FINAL PAGE OF THIS FORM, SELECT DISPOSITION 16 A. REFERAL AND DIVERSION TRIAGE: First, let’s work together to see if Faith Mission’s program is good fit for you. 1. What is your age and date of birth: ________________________________________________________________________________ IF THE INDIVIDUAL IS OVER 18 YEARS OF AGE PROCEED TO QUESTION 2 IF THE INDIVIDUAL IS YOUNGER THAN 18 YEARS PROCEED TO MINOR INDIVIDUAL DIVERSION SCRIPT 2. Do you have any dependent children with you who are also in need of shelter? ____ Yes ____ No IF NO, PROCEED TO QUESTION 3 IF THE INDIVIDUAL ANSWERS YES PROCEED TO YWCA FAMILY CENTER DIVERSION SCRIPT 1
- 20. Faith Mission/Faith Mission Triage Form 3. Where did you stay last night? A. Own Apartment/House B. Friend/Relative C. Hospital/Treatment Facility, if so do you have your discharge paperwork ____ Yes ____No D. Netcare/Mental Health Stabilization E. Other Shelter, please provide the shelter name F. Jail/Prison G. Street/Outside H. Other, please explain IF A PROCEED TO QUESTION 4 IF B, C, D, E, F, G or H IS CHOSEN PROCEED TO QUESTION 5 4. Can you safely stay in your house/apartment tonight? _____ Yes _____ No IF YES, PROCEED TO ELIGIBILITY AND DISPOSITION SECTION ON FINAL PAGE OF THE TRIAGE FORM, SELECT DISPOSITION 3 IF NO, FOLLOW THE SCRIPT IMMEDIATELY BELOW: TRIAGE: Let’s take a look at the situation in your current house/apartment and see if that is a reasonable place for you to stay tonight. A) Have you been evicted from your apartment/home and CANNOT stay in your apartment/house? _____ Yes _____ No IF YES PROCEED TO EVICTION DIVERSION SCRIPT IF NO, PROCEED TO B B) Have the utilities needed to sustain your health and wellbeing (i.e. heat in the winter, electricity or phone for those with serious and/or life threatening health conditions) been disconnected? _____ Yes _____ No IF YES, PROCEED TO QUESTION 5 IF NO, PROCEED TO C, BELOW: C) Are you fleeing a domestic violence situation? _____ Yes ______No IF NO PROCEED TO D, BELOW IF YES AND THE CLIENT IS MALE OR TRANSGENERED PROCEED TO QUESTION 5 IF YES AND THE CLIENT IS FEMALE, PROCEED TO CHOICES ASSESSMENT/DIVERSION SCRIPT D) Is your apartment/house not fit for habitation? _____ Yes _____No IF YES, PROCEED TO UNINHABITABLE DWELLING DIVERSION SCRIPT IF NO PROCEED TO DISPOSITION SECTION ON FINAL PAGE, SELECT DISPOSITION 3 5. Is there a friend or family member you can call right now who would be able to offer you a safe housing option for this evening? _____ Yes _____ No IF NO CONTINUE TO QUESTION 6 IF YES, ALLOW INDIVIDUAL TO MAKE PHONE CALLS (UP TO 3) AND PROCEED TO A, BELOW A) Did individual find shelter with contact? _____ Yes _____ No IF NO CONTINUE TO QUESTION 6 IF YES, PROCEED TO ELIGIBILITY AND DISPOSITION SECTION ON FINAL PAGE, SELECT DISPOSITION 4 6. Are you presently intoxicated? ____ Yes ____ No IF YES, PROCEED TO ENGAGEMENT CENTER ASSESSMENT/DIVERSION SCRIPT IF NO, PROCEED TO QUESTION 7 7. Are you currently having thoughts of harming yourself or someone else? ____ Yes ____ No IF YES, PROCEED TO APPROPRIATE NETCARE DIVERSION SCRIPT IF NO, PROCEED TO QUESTION 8 8. Have you stayed with Faith Mission at any time in the past? ____ Yes ____ No 9. Do you remember when you last stayed with Faith Mission? ____ Yes, Date___________ ____ No 2
- 21. Faith Mission/Faith Mission Triage Form B. DISPOSITION TRIAGE DISPOSITION BASED ON TRIAGE FORM COMPLETION: Select # Disposition Reason Here 1 Referred to Homeless Services in Own State/County/City 2 Referred to Community Assistance Programs, Not In Immediate Need of Shelter 3 Diverted to Own Apartment/House 4 Diverted to Friends/Family 5 Diverted to Huckleberry House and Contacted Children’s Services 6 Individual under 18, Refused Services from Huckleberry House, Provided Contact No.’s and Contacted Children’s Services 7 Diverted to YWCA Family Program 8 Referred to YWCA Family Program, Individual Chose Not to Speak to YWCA at Point of Triage 9 Diverted to CHOICES 10 Diverted to Maryhaven’s Engagement Center 11 Referred to Maryhaven’s Engagement Center, Individual Chose Not to Speak to Engagement Center at Point of Triage 12 Diverted to Netcare 13 Referred to NetCare, Individual Chose Not to Speak to Netcare at Point of Triage 14 Referred to NetCare, Refused to speak to NetCare, Police Contacted 15 Referred to NetCare, Refused to speak to NetCare of Disclose Current Location, No Police Contact Inititated 16 Currently Under Service Restriction 17 ELIGIBLE FOR SHELTER SERVICES 18 Other: 1. Based on completion was client determined to be eligible for Faith Mission program? _____ Yes _____No IF YES AND CLIENT IS PRESENT PROCEED TO ADMISSION REQUIREMENTS, INTAKE AND SERVICE PRESENTATION OUTCOME IF YES, INDIVIDUAL IS ON TELEPHONE AND IT IS BEFORE 8 PM PROCEED TO TRIAGE A SCRIPT BELOW IF YES, INDIVIDUAL IS ON TELEPHONE AND IT IS AFTER 8 PM PROCEED TO TRIAGE B SCRIPT BELOW IF NO, COMPLETE THE FOLLOWING QUESTIONS AND FORWARD TRIAGE FORM TO INTAKE CENTER TRIAGEA: Based on our interview, you are eligible for Faith Mission’s program. You indicated that you are seeking shelter for this evening. While we cannot guarantee you a place in the program, we would like to ensure your place on our reservation list, in order to do that, you need to ensure that you are present at Faith Mission’s shelter (SPECIFY MEN’S OR WOMEN’S DEPENDING ON SHELTER ASSIGNMENT) by curfew in order to secure a bed. Curfew is at 8 PM. TRIAGE B: Based on our interview, you are eligible for Faith Mission’s program. You indicated that you are seeking shelter for this evening. While we cannot guarantee you a place in the program, we would like to ensure your place on our reservation list, in order to do that, you need to ensure that you are present at Faith Mission’s shelter (SPECIFY MEN’S OR WOMEN’S DEPENDING ON SHELTER ASSIGNMENT) as soon as you can, or present at the Intake Center at 315 E. Long at 9:00 AM in the morning. A) Was client diverted or referred to another service? _____ Yes _____No Please provide any additional notes regarding this triage or any unusual incidents that occurred while completing this triage. 3