Drugs acting on skin
•
63 gostaram•13,112 visualizações

Drugs acting on skin and mucous membrane

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Drugs acting on skin
Semelhante a Drugs acting on skin (20)
Último
Último (20)
Drugs acting on skin
- 1. Dr. Mushtaq Ahmed Associate Professor, Pharmacology Punjab Institute Of Medical Sciences, Jalandhar, Punjab
- 3. Interesting Facts about SKIN The largest organ of the body Very important protective layer of the body Also important for: - Thermoregulation - Immunity - Biochemical synthesis & - Sensory functions
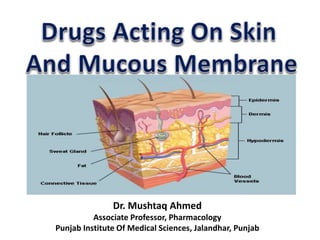
- 4. Structure & function of skin • Skin has two layers → EPIDERMIS & DERMIS: beneath dermis there is fatty tissue • Epidermis, the outer layer contains:- Keratinocytes (keratin), melanocytes (pigment), Langerhan’s cells (antigen), Merkel cells (sensory) • Keratin → present in all the layers of epidermis Abnormal keratin production → psoriasis & icthyotic disorders
- 5. • Superficial keratin layer → stratum corneum • Main function of epidermis → to form stratum corneum • Stratum corneum (horny layer) is important → reducing water loss and prevention of absorption of noxious substances Stratum corneum main barrier for absorption of drugs by topical route Structure & function of skin contd.
- 6. Modes of treatment of skin disorders • Topical • Systemic • Intralesional • Controlled ultraviolet (UV) radiations UV radiations are toxic & can cause sunburn even cancer of skin
- 7. Factors governing rate of absorption of Topical drugs • Thickness of skin • Conc. of drug in vehicle • Degree of hydration Absorption varies in normal skin, damaged skin & exfoliation of skin Transdermal patches → Clonidine (HT), hyoscine (motion sickness) & nitroglycerine (angina pectoris)
- 8. Drugs • Are categorized based on: Action • Vehicles: (powders, greases, ointments, liquids, lotions etc.) • Skin preparations: (adsorbants & protectives, astringents, escarotics, demulcents, irritants & counter irritants ) • Antibacterials, Antifungals, Antivirals • Sunscreens • Keratolytic agents • Corticosteroids Disease or symptoms • Pruritus • Seborrhoea • Alopecia • Leukoderma/Vitiligo • Hyperpigmentation • Scabies/ pediculosis (Ectoparasiticides) • Acne vulgaris • Psoriasis • Atopic dermatitis • Drug induced skin diseases
- 10. Vehicles • Are inert substances which carry the drugs : water content of vehicle very imp. • They also contain some preservatives • Monophasic e.g. powders, greases & liquids • Biphasic e.g. pastes, creams and shake lotions • Triphasic e.g. cream pastes & cooling pastes Vehicle should be non-irritant & cosmetically suitable First pass metabolism in epidermis & dermis also affects the systemic effect
- 11. Powders • Because of soothing & cooling effect → reduce friction by absorbing moisture • Adhere poorly to skin → reduces their usefulness Greases • Petroleum jelly & polyethylene glycol are protective Ointment • Maintain the hydration of stratum corneum Vehicles contd.
- 12. Liquids • Clean and keep the lesion/skin cool • High water content of lotions are also called wet dressings e.g. KMNO4, normal saline Gel & jellies • They are semisolid due to addition of polymers despite containing liquid phase Creams • Oil in water (o/w) type eg. Vanishing/aqueous cream • Water in oil (w/o) type eg. Cold cream Vehicles contd.
- 13. Shake lotions (lotion +powder) • Cause cooling of skin due to evaporation of water Newer Vehicles • Collodions • Liposomes • Microparticle • Transferosomes Vehicles contd.
- 14. Skin Preparations Topical preparations are used for local effect However, TD patches are used for systemic effects Adsorbants and protectives • Bind to noxious and irritant substances on their surface – adsorbant action - Dusting powder, Zinc oxide, Calamine, Talc, Boric acid, polyvinyl polymer, Sucralfate
- 15. Astringents • Tannic Acid - Present in tea, catechu, nutmeg etc. → denaturation of proteins & forms coating - Can be used for bleeding gums (with glycerin) & bleeding piles (as suppository) • Ethanol & methanol - Cause precipitation of proteins and are applied locally for prevention of bed sores and after shave lotion Escharotics (chemical cauterizers) • Cause tissue destruction, sloughing & precipitation of proteins • Used to remove warts, moles, papilloma etc. Phenol, Trichloroacetic acid, silver nitrate, podophyllum Skin Preparations contd.
- 16. Demulcents: Glycerine & propylene glycol • When applied topically they produce soothing effect on denuded mucosa or inflammed skin • Protect the mucous membrane and skin from air and irritant substances Emollients: (wax – hard & soft, paraffin, olive oil etc.) • They produce soothing effect & hydrate the skin • Useful for dry scaly skin Skin Preparations contd.
- 17. Irritants and counterirritants (Nicotinate, salicylate, menthol, camphor, capsaicin) • Irritant substances produce local inflammation, tingling, numbness, cooling or feeling of warmth, hyperaesthesia and vasodilatation • Counterirritants also produce local irritation and relieve pain & inflammation arising from deeper structures • Used for headache, myalgia, neuralgia, joint pain etc. Skin Preparations contd.
- 18. Antibacterial Agents • Common bacterial infections affecting skin: - Furuncle, boil, folluculitis, pyoderma, impetigo, cellulitis etc Antifungal Agents (Benzoic acid) • Common fungal infections- ring worm, oral thrush, dandruff, athlete’s foot Antiviral Agents • Herpes simplex, herpes zoster Chemotherapeutic Agents
- 19. Three types of UV rays: • UVA (Long wave): photoaging/ skin aging (collagen damage), photosesitivity and skin cancer • UVB (medium wave): causes sunburn sun tan, skin cancer & photo aging (skin aging) • UVC (short wave): causes skin injury, sunburn of superficial epidermis Ultraviolet rays & their effect on skin Protection against UV rays: • Avoid exposure to UV rays • Use sunscreens
- 20. Sunscreens • Required to prevent sun burn, aging and skin cancer Classification of sunscreens based on: 1. Physical Action: Titanium dioxide, zinc oxide & calamine They are opaque to all wavelength and reflect them 2. Chemical structure: - PABA & its esters eg. Padimate O - Benzophenones: Avobenzone, oxybenzone, mexenone (highly effective against UVA) - Cinnamates eg. Octyl methoxycinnamate - Salicylates eg. Octisalate - Octocrylene
- 21. Sunscreens contd. 3. Effectiveness against radiation: • Sunscreens for UVA: - Benzophenones eg. Avobenzone, oxybenzone • Sunscreens for UVB: - PABA & its esters eg. Padimate O - Cinnamates eg. Octyl methoxycinnamate - Salicylates eg. Octisalate - Octocrylene Regular use of Sunscreens: reduce risk of actinic keratoses, premature aging and squamous cell carcinoma of skin
- 22. Photosensitivity due to drugs • Systemic use: BZDs, thiazides, hydralazine, sulfonamides, sulfonylurea, NSAIDs, tetracycline, chloramiphenic • Topical use: PABA as sunscreen, musk ambrette (used in perfumes), 6 methyl coumarin (after shave lotion) • Phototoxicity causes severe sun burn • Photoallergy: reaction persists years after the drug withdrawal
- 23. Keratolytic Agents • Used to remove warts and corns, calluses & verrucae • Mild keratolytic Resorcinol and sulphur • Strong keratolytic Salicylic acid, silver nitrate and trichloroacetic acid Some other keratolytic agents: • Lactic, Glycolic & salicylic acid • Propylene glycol • Trichloroacetic acid • Silver nitrate • Urea
- 24. Keratolytic Agents Contd. Salicylic acid • Corneocyte adhesion is reduced by solubilization of intracellular cement • Removes stratum corneum layer by layer Whitfields ointment (salicylic acid 3% & Benzoic acid 6%) Lactic and glycolic acid • Corneocyte adhesion is reduced by disrupting ionic bonds at lowest layer of stratum corneum • Used for xerosis & ichthyosis
- 25. Corticosteroids • Used by both systemic & topical route depending upon disease and severity • Have anti-infammatory and immunosuppressant action • Reduce proliferation of keratocytes, fibroblasts and lymphocytes – antimitotic action • Inhibit migration of inflammatory cells and substances released due to inflammation
- 26. Topical steroids Highest efficacy • Clobetasol propionate 0.05% • Helobetasol propionate 0.05% High efficacy • Betamethasone dipropionate 0.05% • Diflorasone diacetate 0.05% • Fluocinolone acetonide 0.2% & others Intermediate efficiacy • Clobetasol butyrate 0.05% • Hydrocortisone acetate 2.5% • Fluocortolone 0.025% & others Low efficacy • Hydrocortisone butyrate 0.001% • Hydrocortisone acetate 0.1% • Methylprednisolone acetate 0.1% Systemic Agents: Mainly used for serious conditions not responding to other Rx e.g. pemphigus & exfoliative dermatitis Use of Topical Steroids: allergic conditions, infections (bacterial/ viral/fungal), pigment disorders, Psoriasis, Eczematous disorders, drug induced disorders etc
- 27. Topical steroids : ADRs • Infection may spread • Skin atrophy on long term use • Local hirsutism • Depigmentation • Allergic dermatitis • On eyelids – enter eye – glaucoma • Rebound exacerbation of disease after abrupt cessation
- 29. Pruritus • Itching – symptom of many skin diseases • Treatment depends upon cause of pruritus Drugs • Systemic - Antihistaminics - Glucocorticoids • Topical - Corticosteroids e.g. in eczema - Emollient cream, menthol,camphor, phenol, calamine, tar & others
- 30. Seborrhoea • Is due to over-activity of sebaceous glands and skin is greasy → acne, baldness and dermatitis Drugs • Selenium sulphide - Reduces epidermal proliferation & scaling • ketoconazole & corticosteroids Limitation is relapse on discontinuation of the Rx
- 31. Alopecia • Common after age of 40 & about 50% men develop alopecia Drugs • Menoxidil Used topically for the Rx of baldness Possibly acts by ↑ circulation around hair follicles, stimulation of hair follicle reduces the effect of androgen Thickens the hair shafts, ↑ their no. & length Onset is delayed and takes few months Effect is transient- baldness recurs on discontinuation of drug • ADR: Topical- local itching, burning sensation • On significant absorption systemic S/E i.e. tachycardia, palpitation, headache & dizziness
- 32. Alopecia Contd. • Drugs • Finasteride, Dutasteride Type II 5-ᾳ reductase inhibitor There are two types of 5-ᾳ reductase – type I in sebacecious gland & type II present in hair follicles & male genital organ Useful for Rx of baldness, benign hyperplasia of prostrate, prostatic carcinoma Dose: 1mg OD x 2 yrs … minimum effect to come is about 3 months Therapeutic effect is lost one after discontinuation of drug • ADR: • Decreased libido, erectile dysfunction and reduced ejaculate vol.
- 33. Pigment disorders (leukoderma/vitiligo) • Potent photosensitive drug is used with UV rays for vitiligo & psoriasis Drugs • Psoralen, Methoxsalen, Trioxsalen Two types of photoreaction i.e. type I & II take place In type I mono & bifunctional adducts are formed in DNA while in type II sensitized transfer of energy to molecular oxygen ocurs PUVA (Psoralen & UV) facilitates melanogenesis by transferring melanosomes from melanocytes to epidermal cells ADR: Acute: nausea, blistering & painful erythema Chronic: actinic keratosis, photoaging, PUVA lentigins & non melenoma skin cancer
- 34. Hyperpigmentation • Demelanising agents lighten the hyperpigmented patches on skin Drugs - Hydroquinone Inhibits tyrosinase decreases formation & increases degradation of melanosomes Used in melasma, chloasma of pregnancy and sun induced hyperpigmentation - Monobenzone Is toxic to melanocytes – depigmentation is irreversible
- 35. Ectoparaciticides (Scabies & Pediculosis) Scabies • Caused by Sarcoptes scabiei • Itching a common symptom • Female itch mite burrows into superficial layers of skin and lays eggs - form papule – itching (highly contagious) • Drugs are applied topically after a warm scrubbed bath Drugs: Premethrin, Benzyl benzoate, Benzyl hexachloride BHC, IVERMECTIN (only oral drug)
- 36. Ectoparaciticides Scabies & Pediculosis Premethrin • Delays depolarization – neurological paralysis • Effective against scabies (5% cream) & pediculosis (1%) • Absorption – minimal through skin, rapidly metabolized to inactive products • Is safest drug – provides 100% cure For scabies Apply premethrin 5% cream below chin all over the body & left there for 12 h • For pediculosis Apply premethrin 1% cream or lotion for 10 min & then rinse
- 37. Pediculosis • Caused by pediculus captitis (head) • Itching a common symptom Drugs: Premethrin, malathion & DDT • Premethrin is preferred drug • Malathion used in cases not responding to premethrin • DDT - In powder form or solution in kerosine – widely used as insecticide - Not killing ova – disadvantage - Use declined b/o dev. of resistance
- 38. Acne Vulgaris A common skin disorder seen in adolescents (boys & girls) Is due infection of pilosebaceous unit by the bacteria Propionibacium acnes Changes in acne 1. Plugging of hair follicle 2. Accumulation of sebum 3. Growth of Propionibacium acnes 4. Inflammation
- 39. Acne Vulgaris contd. The treatment aims at:- 1. Correction of follicular abnormality 2. Reducing sebum production 3. Controlling infection and 4. Reducing Inflammation Topical Agents o Retinoids Tretinoin, Adaplene, Tazarotene - Normalize the maturation of follicular epithelium & reduce inflammation
- 40. Acne Vulgaris contd. Topical Agents o Antibacterials o Reduce the population of Propionibacium acnes Erythromycin (2-3%), Clindamycin (1%), Benzoyl peroxide (5%) - Combination with retinoids – more effective Other topical agents o Sulfacetamide & it combination with sulfur, Metronidazole and Azelaic acid
- 41. Acne Vulgaris contd. Systemic Agents o Retinoic acid Retinoic acid is vitamin A acid & it possesses vit. A activity in epithelial tissues No activity in other tissues such as eye & germ tissues Rapidly metabolized - eliminated in bile & urine Not stored unlike retinol Its derivatives i.e. tretinoin & isotrtinoin, are used in other conditions o Retinoids o Vit A analogues are called retinoids o Have imp. Role in vision, cell proliferation & differentiation, growth of bone etc.
- 42. Acne Vulgaris contd. Retinoids First generation o Retinol, tretinoin, isotretinoin, alitretinoin Second generation o Etretinate, acitretin Third generation o Tazarotene, bexarotene Retinoid receptors o Retinoic acid receptors (RARs) – subtypes ᾳ, β, ϒ o Retinoid X receptors (RXRs) - subtypes ᾳ, β, ϒ o Out of the above receptors mainly β and ϒ receptors of X receptors are present in human skin 1st & 2nd Gen. retinoids lack receptor specificity – more S/E than 3rd gen. Oral agents – teratogenicity : avoid during pregnancy
- 43. Acne Vulgaris contd. Antibacterials Tetracycline, erytromycin, metronidazole & co-trimoxazole o Reduce p. acnes colonization & also reduce inflammation Hormone and hormone antagonists Oestrogen/ oral contraceptive pills, cypoterone acetate & corticosteriods o Are preferred in case of adult onset acne, premenstrual flares of acne
- 44. Psoriasis • An immunological disorder • Manifests as localized or widespread erythematous scaling lesions or plaques • Increased proliferation, inflammation of epidermis & dermis • Drugs can decrease the lesions but can not cure
- 45. Psoriasis Aim of treatment • To dissolve the keratin & inhibit the further proliferation of cells Topical Agents o Coal tar • Mainly used with UVB – antimitotic effect • Used as solution, gel & shampoo • ADR: folliculitis, irritation, allergic reaction o Calcipotriol (active vit D) • By acting on keratinocytes – causes decrease in proliferation of cultured keratinocytes • By the same mechanism, it produces antipsoriatic effect • Vit D – effective orally & topically Other drugs ; Anthralin, Tazarotene Local Intralesional Photothera py Systemic Method of Treatment
- 46. Systemic Agents • Is required in extensive and severe disease • Cytotoxic & immunosupressants are used Methotrexate • Is a DHFR inhibitor & suppressing immune component cells (mainly T-cells) in Skin • Epidermal inflammation & hyperproliferation are retarded • S/E: bone marrow depression, hepatotoxicity • Other drugs: Hydroxurea, Cyclosporine, Efalizumab, • Liarozole & rambazole- newer agents Psoriasis Contd.
- 47. Atopic Dermatitis • Is an inflammatory condition of skin – starts during infancy & childhood – may persist upto adult age • Allergens & environmental pollutants may cause the disease • Itchy papules & plaques – characteristics of this condition • Treatment : Glucocorticoids, antihistaminics, immunosupressive agents
Notas do Editor
- Trichloroacetic acid, silver nitrate, podophyllum : are also keratolytic agents