Wellness couchevalauation
•
0 likes•170 views

for more information contact freddy on mofreddy@facebook.com or inbox freddy moraloge on facebook

Recommended
More Related Content
Similar to Wellness couchevalauation
Similar to Wellness couchevalauation (20)
More from fred fred
More from fred fred (20)
Recently uploaded
Recently uploaded (20)
Wellness couchevalauation
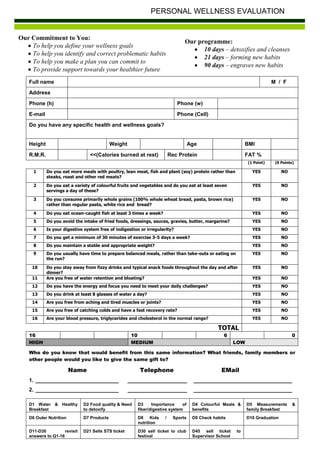
- 1. PERSONAL WELLNESS EVALUATION Our Commitment to You: Our programme: To help you define your wellness goals 10 days – detoxifies and cleanses To help you identify and correct problematic habits 21 days – forming new habits To help you make a plan you can commit to 90 days – engraves new habits To provide support towards your healthier future Full name M / F Address Phone (h) Phone (w) E-mail Phone (Cell) Do you have any specific health and wellness goals? Height Weight Age BMI R.M.R. <<(Calories burned at rest) Rec Protein FAT % (1 Point) (0 Points) 1 Do you eat more meals with poultry, lean meat, fish and plant (soy) protein rather than YES NO steaks, roast and other red meats? 2 Do you eat a variety of colourful fruits and vegetables and do you eat at least seven YES NO servings a day of these? 3 Do you consume primarily whole grains (100% whole wheat bread, pasta, brown rice) YES NO rather than regular pasta, white rice and bread? 4 Do you eat ocean-caught fish at least 3 times a week? YES NO 5 Do you avoid the intake of fried foods, dressings, sauces, gravies, butter, margarine? YES NO 6 Is your digestive system free of indigestion or irregularity? YES NO 7 Do you get a minimum of 30 minutes of exercise 3-5 days a week? YES NO 8 Do you maintain a stable and appropriate weight? YES NO 9 Do you usually have time to prepare balanced meals, rather than take-outs or eating on YES NO the run? 10 Do you stay away from fizzy drinks and typical snack foods throughout the day and after YES NO dinner? 11 Are you free of water retention and bloating? YES NO 12 Do you have the energy and focus you need to meet your daily challenges? YES NO 13 Do you drink at least 8 glasses of water a day? YES NO 14 Are you free from aching and tired muscles or joints? YES NO 15 Are you free of catching colds and have a fast recovery rate? YES NO 16 Are your blood pressure, triglycerides and cholesterol in the normal range? YES NO TOTAL 16 10 6 0 HIGH MEDIUM LOW Who do you know that would benefit from this same information? What friends, family members or other people would you like to give the same gift to? Name Telephone EMail 1. ____________________________ ____________________ _________________________________ 2. ____________________________ ____________________ _________________________________ D1 Water & Healthy D2 Food quality & Need D3 Importance of D4 Colourful Meals & D5 Measurements & Breakfast to detoxify fiber/digestive system benefits family Breakfast D6 Outer Nutrition D7 Products D8 Kids / Sports D9 Check habits D10 Graduation nutrition D11-D30 revisit D21 Sells STS ticket D30 sell ticket to club D45 sell ticket to answers to Q1-16 festival Supervisor School