
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (19)
Destaque
Destaque (20)
Semelhante a Voltage-Gated Ion Channels and Disease
Semelhante a Voltage-Gated Ion Channels and Disease (20)
Voltage-Gated Ion Channels and Disease
- 1. Diomedes E. Logothetis - November 15, 2007 Voltage-Gated Ion Channels and the Action Potential Ion Channels and Disease Lecture goals: The first part of this lecture will use our understanding of voltage-gated channel function to explain how an action potential is generated and conducted. Examples such as the synapses between neurons or between neurons and muscle are examined. The second part of the lecture will use examples of ion channelopathies. Ion channel disorders lead to the following conditions listed alphabetically: Autoimmune disorders, Bipolar disorder, Cancer, Cardiac arrhythmias and sudden death, Cystic fibrosis, Diabetes, Epillepsy, Myotonias, Nephropathies and Pain. We will examine a couple examples to illustrate how defects in ion channel function leads to disease. Learning Objectives 1. Describe the ion substitution experiments performed by Hodgkin and Huxley in elucidating the ion responsible for the biphasic currents obtained in their voltage clamp experiments with the squid giant axon. What pharmacological agents can also distinguish between these currents? 2. Know how to plot and explain the current-voltage relationship of voltage-gated K+ and Na+ currents. 3. Contrast the topology of various voltage-gated channels and discuss their distinguishing structural feature involved in voltage sensitivity. 4. Know how voltage dependence is recognized in single-channel records obtained from voltage steps to different potentials. Predict the result of an ensemble average of many single-channel current records in response to steps to a particular voltage. 5. Predict the result of an ensemble average of many single-channel current records in response to steps to a particular voltage. 6. Plot the probability of Na+ channel opening and the Na+ current obtained as a function of voltage. 7. Describe an action potential in terms of its dependence on the time course of gNa and gK. 8. Discuss the mechanism of Na+ channel inactivation and its control of the refractory period for generation of multiple action potentials. 9. Describe the events taking place in the neuromuscular junction leading to an action potential. 10. Physiologic Principles Underlying Ion Channelopathies 11. Examples of ion channel dysfunction leading to disease (The TRP channel family and CFTR) Reading • Lecture Notes (will be provided in advance of the lecture) • Alberts B., Johnson A., Lewis J., Raff M., Roberts K., Walter P. Molecular Biology of the Cell. Fourth Edition, Garland Science. Chapter 11, For extracellular ligand-gated channels see pp. 637-657. • Review papers: Cannon SC. Physiologic Principles Underlying Ion Channelopathies. Neurotherapeutics 2007 4:174-183 • Nilius B, Owsianik G, Voets T, Peters JA. Transient receptor potential cation channels in disease. Physiol Rev. 2007 Jan;87(1):165-217. Review Campbell JN, Meyer RA. Mechanisms of neuropathic pain. Neuron. 2006 52(1):77-92. Review Ashcroft FM. From molecule to malady. Nature. 2006 Mar 23;440(7083):440-7. Review 1
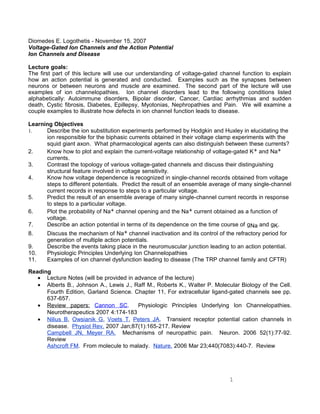
- 2. VOLTAGE-GATED CHANNELS We are now ready to consider voltage-gated ion channels, the class of ion channels that generate action potentials, the brief electrical signals by which excitable cells such as neurons, muscle and endocrine cells communicate with one another. I will present voltage-gated channels with a historical perspective, to underscore the monumental work of two British scientists, Hodgkin and Huxley (Nobel laureates 1963) whose work has influenced physiologists in as major a way as Watson and Crick influenced molecular biologists. Hodgkin and Huxley, used the voltage clamp technique to study a relatively easy preparation, the squid giant axon. The experiment shown in Fig. 1 illustrates the currents they obtained using different voltage clamp protocols. A hyperpolarizing step from -65 mV (resting potential) to -130 mV failed to produce a sizable ionic current (Fig. 1A). In contrast when the axon was depolarized to 0 mV, a large transient inward current and a later outward sustained current was elicited. The ionic permeability of the membrane was changed in a dramatic manner by the step depolarization. Hodgkin and Huxley set out to determine which ions carry the current and how the underlying membrane permeability mechanisms work. First they reasoned that each ion seemed to move passively down its electrochemical gradient, so basic thermodynamic arguments could be used to predict whether the net movement of an ion would be inward or outward at a given membrane potential. For example current carried by Na ions should be inward at potentials negative to the equilibrium potential ENa, and outward at potentials positive to ENa. If the membrane was voltage clamped to ENa, Na ions should make no contribution to the membrane current, and if the current reverses sign around ENa, it is possibly carried by Na ions. The same argument could be applied to K+ , Ca2+ , and Cl- . Second, ions could be easily added to or removed from the external solutions. In the extreme, if a permeant ion were totally replaced by an impermeant ion, one component of current would be abolished. Using these approaches Hodkin and Huxley in 1952 identified two major components, INa and IK, in the ionic current. They first noticed that the early transient currents reverse their sign from inward to outward at around +60 mV (also referred to as the "reversal potential") as would be expected if they are carried by Na ions. The late currents, however, are outward at all test potentials (more positive to -65 mV), as would be expected for a K current with a reversal potential more 2 Figure 1. An axon is bathed in sea water and voltage- clamped by the axial wire method. The membrane potential is held at –65 mV and then hyperpolarized in a step to –130 mV or depolarized in a step to 0 mV. Outward ionic current is shown as an upward deflection. The membrane permeability mechanisms are clearly asymmetrical. Hyperpolarization produces only a small inward current, while depolarization elicits a larger and biphasic current.
- 3. negative than -65 mV. The identification of INa was then confirmed by replacing most of the NaCl of the external medium by choline chloride (Fig. 2). The early inward transient current seen in the control ("100% Na") disappears in low Na ("10% Na"), while the late outward current remains. Subtracting the low-Na record from the control record reconstructs the transient time course of the Na+ current, INa, shown below. The properties of INa and IK are frequently summarized in terms of current-voltage relations. Figure 3 shows the peak INa and the late IK plotted as a function of the voltage-clamp potential. With modern terminology we would describe the Hodgkin and Huxley results to indicate that the axon membrane has two major types of ionic channels: Na channels with a positive reversal potential, ENa, and K channels with a negative reversal potential, EK. Both channels are largely closed at rest and they open with depolarization at different rates. Nowdays, pharmacological tools exist to isolate Na from K current. Tetrodotoxin (TTX), a paralytic poison of some puffer fish, block selectively Na channels. Tetraethylammonium ion (TEA) selectively blocks IK. Figure 4 shows a family of voltage steps producing a family of curents before and after application of the selective blockers. It is from traces like these that I-V curves are constructed. 3 Figure 2. An illustration of the classical ionic substitution method for analyzing the ionic basis of voltage-clamp currents. Ionic currents are measured in a squid axon membrane stepped from a holding potential of –65 mV to –9 mV. The component carried by Na+ ions is dissected out by substituting impermanant choline ions for most of the external sodium. (a) The voltage protocol applied to an axon in seawater, showing inward and outward ionic currents. (b) Axon in low-sodium solution with 90% of the NaCl substitued by choline chloride, showing only outward ionic current. (c) Algebraic difference between experimental records A and B, showing the transient inward component of current due to the inward movement of external Na+ ions. a. b. c. Figure 3. The axon membrane potential is stepped under voltage clamp from the negative holding ptential (VH or EH) to various test potentials. Peak transient sodium current and steady-state potassium current from each trace are polotted against the test potential. The curvature of the two I-E relations between –50 to –20 mV reflects the voltage- dependent opening of Na and K channels.
- 4. Voltage-gated channels are comprised of four (six membrane-spanning-segment) subunits as compared to the inward rectifier K channels (having only two membrane-spanning-segments) as we discussed in the last lecture. K channels are coded in single subunits just like the CNG channels. Na and Ca voltage-gated channels exist as four-subunit transcripts all coded in a single gene. What characterizes voltage-gated K channels from other channel proteins is a unique motif found in the fourth transmembrane domain (S4), where in this predicted α helix every third amino acid residue is a positively charged arginine or lysine. Strong evidence has implicated this segment as an integral part of the molecular voltage sensor that upon depolarization moves away from the internal membrane surface and pulls the gate open allowing ions to flow down their electrochemical gradient (Fig. 5). 4 Figure 4. Pharmacological dissection of INa and IK. A node of Ranvier under voltage clamp is held at –95 mV, hyperpolarized for 40 ms to –120 mV, and then depolarized to various potentials ranging from –60 to +60 mV in 15-mV steps. (A) Normal INa and IK in Ringer’s solution. (B) Same node after external addition of 300 nM TTX. Only IK remains. (C) Control measurements in another node. (D) Same node after external addition of 6 mM TEA. Only INa remains. Figure 5. Topology of the intracellular ligand-gated channels we considered in the last lecture, compared to voltage- gated channels discussed in this lecture. Each of the four subunits in these channel proteins is thought to contain either two (M1-M2 for inward rectifier K channels) or six membrane-spanning α helixes, S1-S6. In voltage-gated channels the S4 segment contains several positively charged amino acids and is the voltage-sensing α helix. The pore-lining P segment lies between S5 and S6. The N-terminus of the polypeptide, located in the cytosol, contains a globular domain essential for inactivation of the open channel.
- 5. Channel gating underlies variable conductance As mentioned above, ion channels fluctuate between open and closed states, the process we have called channel gating. With patch clamp recording, it has been possible, to measure the openings and closings of a single channel molecule directly. Figure 6 shows such recordings from a tiny "patch" of membrane that contains just one voltage-gated K-channel. Two voltage steps are shown, one at -20 and the other at +20 mV. The current level fluctuates between the zero current level (closed channel) and a distinct open level. As expected for a K channel, the current through the open channel is outward at both potentials, but the outward current is larger at +20 mV. The other important difference between the two current traces is the fact that the channel is open more often at the positive potential. The fraction of time a channel spends in the open state is called the open probability Po (Po ranges between 0 and 1). Figure 6. Single channel recordings from a voltage-gated K+ channel. The step to +20 mV elicits single channel currents of larger amplitude that the step to -20 mV, simply because of the greater driving force. Similarly, the step to +20 mV shows that the channel spends more time in the open state that it does during the step to -20 mV. It is precisely this increase in open probability seen at more depolarized voltages that characterizes these channels as voltage sensitive. Below in Figure 7 we see records from a patch-clamp experiment, where a single voltage- gated K+ channel has been isolated (e.g. in the on-cell, inside-out or outside-out modes). The membrane voltage is clamped between two levels, first at –100 mV for a relatively long period of time and next to +50 mV for 40 ms. Below we see the gating of a single K+ channel in response to this voltage step repeated nine times (top trace). Each voltage step produces a current record as shown in each of the records shown below. The dashed line indicates the zero current level (the channel is closed), while the transition to the positive current indicates the potassium flow for as long as the channel stays in the open position. Each time the channel opens and closes stochastically. This probabilistic nature of ion channel activity is very representative of single molecular function at large. If we were to signal average current records obtained from a voltage step of the membrane to the same value repeated many times (e.g. forty times in this example), we would obtain the ensemble average record shown at the bottom of the figure. This macroscopic record is identical to what one would obtain if forty K+ channels were to open simultaneously during a voltage step to the same potential. 5
- 6. Figure 8 shows recordings of single Na+ channels in response to a voltage pulse. Notice that currents are elicited with a smaller delay than K+ currents, they activate more rapidly than K+ currents and inactivate despite the maintenance of the depolarizing stimulus, a phenomenon termed inactivation (more about inactivation below). 6 Figure 7. Gating in single K+ channels. (a) Nine consecutive depolarizations yield non-inactivating K+ channels. Notice the channel re-openings and the relatively long times for the first channel opening following the voltage stimulus (compare to figure 8 showing single Na+ channel activity). (b) Ensemble average of 40 repeats of the same protocol. (From Hille: Ionic Channels of Excitable Membranes, 1992, Sinauer Press, p. 69) Figure 8. Cell-attached patch-clamp recording of unitary Na currents in a toe muscle of adult mouse during a voltage step from -80 to -40 mV. (A) Ten consecutive depolarization steps. One can see two superimposed channel openings in the first record but not in any of the others. Dashed line indicates the current level when Na channels are closed. (B) The ensemble mean of 352 repeats of the same protocol. (From Patlak and Ortiz, from Hille: Ionic Channels of Excitable Membranes, 1992, Sinauer Press, p. 68)
- 7. Figure 9 shows the behavior of macroscopic Na currents (top two panels) and compares it to that of the total current in a neuron (containing K+ channels as well – bottom panel). If we were to plot the normalized current as a function of voltage (maximum current at 0 mV would be 100%) we can obtain a plot of the probability that Na+ channels would be open at a given membrane potential (top panel). If we were to plot the macroscopic current flowing through many Na+ channels, as a function of the membrane voltage steps that we clamp the plasma membrane, we would obtain the I-V plot shown in the middle panel. Many mechanisms exist which can alter Po in an ion channel. For the ion channels, which generate the action potential, the most important regulator of Po is the transmembrane voltage (membrane potential). These voltage-gated ion channels, contain as we mentioned earlier a voltage sensor connected to a "gate", which keeps the channel shut at negative potentials and opens it at more positive potentials. It is this voltage dependent change in Po of Na and K channels that underlies the conductance changes which lead to the nerve action potential. Note that a change in membrane potential has two independent effects on voltage-gated channels: (1) It changes the driving force for ion movement and thus the current through an open channel. (2) It changes the open probability Po. The voltage dependence of Po for voltage-gated Na channels is shown in the top panel of Fig. 9. The second panel shows the voltage dependence of the Na current where we have now scaled the maximum conductance gmax (conductance of an open Na channel) with Po to obtain INa=gmax Po (V-VNa). The third panel of Fig. 9 finally shows the net membrane current as the sum of the Na channel properties and the conductance of the resting membrane (mainly K channels). For simplicity's sake we have not taken into account that Po for K-channels is also voltage dependent. The net ionic membrane current has an N-shaped form with three intersects of the zero-current axis. We will examine this panel in greater detail below in an attempt to determine the threshold for action potential generation. For now, let us just consider the strikingly different effects of an increase in the Na or K conductance by membrane depolarization: 7 Figure 9 The open probability (Po) of Na channels increases steeply with depolarization. Thus, the effective Na conductance is voltage dependent. The sodium current INa= gNa (V-VNa) with its voltage dependent conductance gNa= gmax Po. gmax is the (maximal) conductance of a Na channel when Po = 1. Net ionic current, obtained as the sum of the Na current and the current through the resting membrane, here represented as IR=gR (V-VR). Note N-shaped form with three zero-current intersects. Middle intersect is threshold; more about that in figure 13.
- 8. Thus, a depolarization which activates only K channels terminates itself (negative feedback) whereas a depolarization which activates Na channels becomes regenerative through positive feedback between depolarization and further opening of Na channels. This positive feedback leads to the explosive upstroke of the action potential, once the threshold is reached (see below). The last property of Na channels necessary for the understanding of the action potential is Na channel inactivation. The voltage dependent increase of the opening probability of Na channels is not maintained in time, but is rapidly transient. When Na channels are depolarized rapidly, but then held at a positive potential, they open first but then enter soon a non conducting "inactivated" state (see Fig.8). The word "inactivated" means that as long as a Na channel is in that state, it cannot be opened again by a subsequent depolarization. This property of Na+ channels is an important factor in terminating the action potential (along with the K+ channel mediated hyperpolarization). A cartoon of the three important functional states of a voltage gated Na-channel is shown in Fig. 11. Return of Na channels from the inactivated to the resting (closed) state requires repolarization of the cell membrane. Another action potential can only be elicited after a large fraction of Na channels have returned from the inactivated to the resting state, i.e. the Na channels have become available to open once again. The time necessary for this recovery from inactivation determines the so called "refractory period", the minimal time required before the cell can be excited again to fire the next action potential. In nerve and muscle cells, this refractory period is very short (a few milliseconds) but it is greatly prolonged in heart cells. Because inactivation of Na channels during the action potential shuts down 8 Figure 11. Ball-and-chain model of inactivation gating. Three gating states of the channel: Resting (R), Open (O) and Inactivated (I). The part of the channel that interacts with the inactivation ball becomes exposed only upon opening of the channel. Figure 10
- 9. the inward current carried by those channels, Na channel inactivation helps terminate the action potential. Maintained depolarizations will tend (after an initial Na channel opening) to drive Na channels into the inactivated state and therefore render a cell unexcitable. The relative number of resting versus inactivated Na channels is steeply voltage dependent between -80 and -40 mV, so steady depolarizations in this potential range will greatly reduce the number of available (resting) Na channels, and therefore the excitability of a cell. An example of a clinically important case of maintained depolarization is that of elevated serum potassium levels. Variable conductances: the generation of the action potential When excitable cells are depolarized from their resting potential beyond a certain level (threshold – more about this in figure 13), they respond with a relatively large, stereotyped potential change, the action potential. It is the action potential propagating away from the site of origin, which underlies impulse conduction in nerve, muscle and heart. We will deal with impulse conduction below but first let us consider the ionic basis for the generation of the action potential. Figure 12 shows the typical configuration of a nerve action potential. An initial depolarization from the resting potential leads into a very rapid depolarization, called the upstroke of the action potential. After the upstroke, the action potential peaks at a value positive to +30 mV and then repolarizes. In many cells repolarization is followed by an "undershoot" (afterhyperpolarization) of the membrane potential, which returns to its resting value a few milliseconds after the end of the action potential. How can an action potential be triggered? Where does the initial depolarizing stimulus come from in a real cell that triggers an action potential? The depolarizing stimulus can come from two sources. 1. Through electrical connections: From a cell that generates its own action potentials (i.e. a pacemaker cell – such as in the heart or some neurons) and through specialized channels called gap junctions (that connect pacemaker cells to other non-pacemaking cells - see last lecture) current travels from one cell to another depolarizing the membrane and triggering an action potential. This is equivalent to injecting current through a microelectrode into a cell. 9 Figure 12 We have seen in the last paragraph that the membrane potential is determined by the relative conductances of the ion channels in the cell membrane. ~45 years ago Hodgkin and Huxley concluded that the nerve action potential is generated by rapid conductance changes of Na and K channels. For this work which was the first successful utilization of the voltage clamp technique Hodgkin and Huxley received the Nobel Prize in 1963. In the presence of Na and K channels, the membrane potential can swing between VK=-90 mV and VNa=+60 mV as these channels open. At rest, gK>>gNa, and V is just slightly more positive than VK. Upstroke and peak of the action potential are the result of a massive increase of gNa, such that at the peak of the action potential the membrane potential approaches VNa because now gNa>>gK. Repolarization occurs because gNa falls back to its resting low level and gK increases. The resulting afterhyperpolarization marks the closest agreement between V and VK, at this time gK>>>gNa. As gK returns to its normal level, V depolarizes to the resting level. The timecourse of the changes in gNa and gK underlying the generation of the nerve action potential is also shown in the bottom panel.
- 10. 2. Through other channels: The initial depolarization can come from other channels, for example channels opened by neurotransmitters. Those could be the extracellular ligand-gated (neurotransmitter-activated) ion channels we encountered in the last lecture, such as the nicotinic acetylcholine receptor (AChR). This channel is opened by the binding of two acetylcholine molecules and acts to depolarize the membrane of a skeletal muscle fiber (see last lecture). It is about equally permeable to both K+ and Na+ , so its equilibrium (or reversal) potential is near 0 mV. This means that it would carry inward current when V<0 mV, for example at the resting potential. Another way to think about it is that near the resting potential there would be less driving force for K+ ions to leave the cell (closer to VK) than for Na+ ions to enter the cell (farther away from VNa). So when AChR channels open and the cell is at the resting potential, there will be a net inward current that can cause the initial depolarization that brings the cell membrane to the threshold potential. Cell capacitance, the metabolic cost of an action potential and The capacitance of a membrane determines the metabolic "cost" of an action potential, because as you may remember from my first lecture, the higher the capacitance, the more charge must be moved to generate the voltage of an action potential. The charge is supplied by the ionic current, and the greater the current, the more energy must be expended by the Na/K ATPase (see next lecture) to restore the ion gradients. Since the specific capacitance of a lipid bilayer is fairly constant at 1 µF/cm2, we can calculate the number of Na ions, which have to enter a cell to produce the typical depolarization of ~ 100 mV associated with the action potential upstroke. Let's assume a spherical cell (e.g. a nerve cell body) with a diameter of 20 mm. Membrane area = 4πr2 = 1267 mm2 Capacitance = 1267 µm2 x 1 µF/cm2 = 12.67 pF (1pF = 10-12F) Charge = 12.67 pF x 100 mV = 1.267 x 10-12 C Each Na ion carries the elementary charge of 1.6 x 10-19 C, so 1.267 x 10-12 C/1.6 x 10-19 C/Na ion = 7.91 x 106 Na ions/action potential. Will this lead to a measurable increase of the intracellular Na concentration? Our cell has a volume of 4/3pr3 = 4187 mm3. At [Na]i= 15mM the cell contains 0.015 moles/liter x 6x1023 ions/mole x 4187x10-15 liter = 3.77 x 1010 Na ions/cell So, each action potential will increase [Na]i by about 0.05 %, an increase that is not measurable chemically. After prolonged activity however, i.e. hundreds of action potentials, [Na]i will start rising and active pumping is required to maintain the transmembrane gradient. The relative change in ion concentration produced by each action potential also varies with the surface to volume ratio of a cell. Since in our example we have chosen a spherical cell (minimal surface to volume ratio), the relative Na accumulation can be higher in cells of different geometries. Example of Ion Channels in Disease CFTR channel mutations lead to cystic fibrosis: The cystic fibrosis transmembrane regulator (CFTR) encodes for a chloride channel. CFTR is a member of the ABC transport proteins that possesses two nucleotide binding folds (or domains) (NBFs or NBDs). 10
- 11. In addition to the two NBDs, CFTR also possesses a unique Regulatory (R) domain. The main function of the R domain seems to be to inhibit ATP binding to the NBDs. Phosphorylation of the R domain, predominantly by cAMP-dependent Protein Kinase A removes the inhibitory action of the R domain on ATP binding to the NBDs. ATP binding (and possibly ATP hydrolysis) to the NBDs is responsible for channel gating. It has been proposed that ATP binding to the first NBD (NBD1) gates the channel open, while binding of a second ATP molecule to NBD2 shuts the channel off. Cystic fibrosis may be caused by any of the more than 730 mutations of CFTR which have been described so far. The most prevalent mutation (~70% of the cases) is the deletion of phenylalanine 508 which prevents proper folding of the channel and its targeting to the cell surface. The consequence of disrupting Cl- channel function is a defect in NaCl transport in both epithelial and non-epithelial tissues. Let us consider secretion and absorption of NaCl in epithelial cells. Both secretion and absorption of NaCl are basic functions of epithelial cells. This transport processes require polarized insertion of proteins specialized in ion transport to either the apical (luminal) or the basolateral membranes of epithelial cells. In order to effectively transport NaCl from the apical to the basolateral side, or vice versa, the task of all participating transporters needs to be coordinated. Membrane transporters and pumps communicate through changes of intracellular ion concentrations, as well as by common intracellular second messenger pathways. In this respect, crosstalk between the basolateral and luminal membranes of epithelia has become an important issue in the understanding of transepithelial NaCl transport. Secretion and absorption of NaCl can be localized in separate types of epithelial cells where there is a local separation of the two processes. Yet, in certain airway and colonic epithelial cells secretion and absorption of NaCl can occur through the same cells. Secretion in the net transfer of NaCl from the basolateral side to the luminal side of the epithelial cell. Secretory epithelial cells contain an active Na 2Cl K cotransporter in the basolateral membrane, by which Cl together with Na and K are taken up from the basolateral side into the cell. The K that enters in this way can exit the cell from either K channels in the basolateral membrane or K channels in the apical side. The Na entering through the cotransporter exits through the Na/K-ATPase in the basolateral membrane. In a stimulated airway or colonic epithelial cell (by agonists that produce elevated levels of cAMP), the Cl that entered through the contransporter exits the cell from the apical side predominantly through CFTR channels. Active CFTR channels block the activity of Na channels also found in the apical side of the epithelial cell. Thus a net secretion of NaCl is accomplished when CFTR channels are fully active. In the case of an unstimulated epithelial cell the CFTR activity is not sufficient to inhibit the epithelial Na channel on the apical surface. Therefore, there is a significant influx of Na from the luminal side to the inside of the cell. This Na leaves the cell through the basolateral side via the Na/K ATPase. Due to the change in intracellular Na concentration effected by Na transport through the epithelial Na channel the Na 2Cl K cotransporter is no longer functional. Cl transport is now reversed from the luminal to the basolateral side through CFTR or other Cl channels present on the apical and basolateral sides. Therefore, in this case we have a net absorption of NaCl from the luminal to the basolateral side. In cystic fybrosis the CFTR channels are defective in being activated by cAMP-dependent protein kinase and therefore there is always NaCl absorption rather than secretion. In other words, airway and colonic epithelial cells fail to switch from absorptive to secretroy. As a consequence of this defect, enhanced paracellular and trancellular water flux from the luminal to the basolateral side of the epithelium will dehydrate airways resulting in the well described pathophysiological consequences of enhanced mucus viscocity, decreased mucociliary clearance and bacterial colonization of the airways. 11
- 12. 12