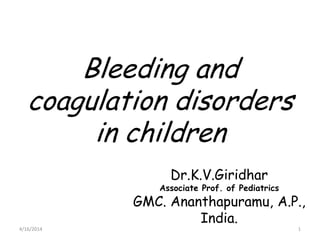
5. THE CLOTTING MECHANISM
INTRINSIC EXTRINSIC
PROTHROMBIN(II) THROMBIN(III)
FIBRINOGEN
FIBRIN
(I)
V
X
Tissue ThromboplastinCollagen
VIIXII
XI
IX
VIII
VII
PT
PTT Vit.K, Live
r
9. Vessel Abnormalities
• increased vascular fragility
• manifest by petechial hemorrhages of skin/mucous
membranes
• not life threatening bleeding
1. congenital: a. Ehlers-Danlos syndrome (AD)
b. hereditary hemorrhagic telangiectasia (AD)
2. acquired: a. hypersensitive vasculitis
(i) drug reaction : immune complex deposit in
vessel walls(Thaizide diuetics)
(ii) Henoch-Schonlein purpura
b. scurvy (vit C deficiency)
Lab: BT, Plt count, PT, PTT will be normal
10. VESSEL WALL ABNORMALITIES:
EHLERS DANLOS DISEASE:
• Congenital disorder of collagen
synthesis
• in which capillaries are poorly
supported by s/c collagen
• ecchymosis are commonly
observed.
11. VESSEL WALL ABNORMALITIES:
HERIDITARY HEMORHAGIC TELANGECTSIASIS
• Dominant inherited condition.
• Telengectias, are small aneurysms found on
finger tips, face, nasal passages, tongue
and GIT.
• few people develop pulmonary A/V
malformation.
• Pt. develops recurrent bleeding/epistaxis/
occult GIT bleeding, leads to Iron def.
anemia
Rx.
• Iron therapy for blood loss.
• Local cautery/laser therapy for single lesion
• Estrogens may be tried.
14. QUANTITATIVE PLATELETS DISORDER
(Thrombocytopenia)
Mechanisms:
1 Failure of megakaryocytic maturation.
2 Excessive platelets consumption after their
release into circulation i.e ITP, DIC etc.
3 Platelets sequestration in enlarged spleen
i.e HYPERSPLEENISM.
S/S:
· Petechial cutaneous bleeding, intracranial
bleeding and oozing from mucus membrane
& skin surface.
· Lab: decreased platelets count and
prolong bleeding time.
15. (Thrombocytopenia) Causes:
Marrow Disorder
Aplastic anemia
Hem. malignancy
Myelodysplastic
disorder
B12 deff.
Non Marrow Disorder
Immune disorders
ITP, Drug induced
Sec: ALL, SLE
Post transfusion
DIC, TTP
HU
syndrome, Hyperspleenism
Heamangiomas
Sepsis
Viral infection
Management:
Rx Underlying cause
Platelet transfusion
16. IDIOPATHIC THROMBOCYTOPENIC
PURPURA(ITP)
• An autoimmune antibody IgG is
formed against unknown antigen of
platelets membrane/surface.
• Antipletelet antibody binds to
complement, but platelets are not
destroyed by direct lysis.
• Destruction takes place in
spleen, where spleenic macrophages
destroyes antibody coated platelets.
17. IDIOPATHIC THROMBOCYTOPENIC
PURPURA. (Clinical Features)
In Children(acute):
Often precipitated by viral infection and
usually self limited
Asymptomatic not febrile.
Present with mucosal/skin
bleeding, mennorrhagia, purpura, petechiae
.
Adults(chronic):
Commonly affects female.
Ratio 2:1 (male/female ratio)
18. IDIOPATHIC
THROMBOCYTOPENIC PURPURA.
Δ LAB:
platelets below 10,000 /ml.
Bone marrow will appear normal.
Rx
PREDNISONONE: 1-2 mg/kg/day.
Immunoglobulin: 1g/kg/day 2-3 days.
DANAZOLE: 600mg/day response rate is 50%
IMMUNOSUPPERESSIVE DRUGS: i-e
vincristine, vinblastine, azathioprine, cyclosprin,
cyclophosphomide.
SPLEENECTOMY:
Prognosis:
The prognosis will be good, if disease is initially
controlled with prednisolone,
spleenectomy is definite Rx.
21. QUALITATIVE PLATELET DISORDER
BERNARD SOULIER SYNDROME:
Autosomal recessive intrinsic platelets disorder.
Due to lack of glycoprotein (Gp1b), receptor for
vonWillibrand‟s factor.
Clinical Features:
Presents with mucosal bleeding and post operative
oozes.
LAB:
Thrombocytopenia may be present, and Plt.s are
abnormally large in size.
BT is prolonged
Von Willibrand’s factor Normal
Rx:
Platelet transfusion
22. QUALITATIVE PLATELET DISORDER
GLANZMANN’s THROMBASTHENIA:
Autosomal recessive disorder.
Lack of receptors (glycoprotein Ib & IIIa)
for fibrinogen on platelets.
Platelets fails to aggregate in respons to
ADP, collagen, thrombin.
Clinical Features: Mucosal bleeding
LAB:
Platelets no‟s and morphology are normal
B.T is prolonged
Rx:
Platelet transfusion
23. QUALITATIVE PLATELET DISORDER
VON-WILLIBRAND’S DISEASE:
• Autosomal dominant(gene for vWF is
located on chromosome 12.)
• vWF is synthesized by endothelial
cells and megakaryocytes
• It acts as carrier protein for factor
VIII by non-covalent bond. A defect
therefore leads to decreased plasma
factor VIII level.
• It also forms bridges b/w platelets
and sub endothelium.
• There fore defect of vWF leads to
prolonged bleeding.
24. VON-WILLIBRAND’S DISEASE:
Clinical Features:
• Mucosal bleeding (mild-massive)
LAB:
• Reduced level of vWF which often accomplished
by sec: reduction in factor VIII and prolonged
bleeding time (B.T)
Rx:
• MILD HAEMORRHAGES:
Desmopressin 0.3 μg/kg, after which vWF levels
usually raise 3 in 30-90 minutes
• MASSIVE HAEMORRHAGES:
Factor VIII
25. COAGULATION DISORDER:
Coagulation factor disorder can
either due to single factor def., i.e.
a “congenitaldeficiency”, eg factor
VIII resulting in HAEMOPHILIA-A
or due to multiple factor def., which
is an „‟acquired” eg Sec: to liver
disease or warfarin therapy.
28. HEAMOPHILIA – A (CLASSIC TRUE
HAEMOPHILIA)
• X-linked disorder
• Due to deff. of factor VIII
C/F:
• Bleeding occurs as bruising at the age of 6 months.
• Trauma results in excessively bleeding.
• Recurrent bleeding /hemorrhage in
knee, elbow, ankle, and hip. (Hemarthrosis)
• Mucus membrane /internal bleeding of
mouth, lips, gums, brain and kidney also occur
• Muscle haematoma esp. calf and Psoas muscle
Rx
• Factor VIII infusion
30. HAEMOPHILLIA – B (CHRISTMAS
DISEASE)
• Due to deff: of factor IX
S/S:
• Same in type A
Rx
• Factor IX infusion
LONG TERM COMPLICATION
COMPLICATION due to repeated hemorrhage:
• Arthropathy of large joints eg knee, elbow
• Muscle atrophy due to haematoma
• Mononeuropathy due to pressure of haematoma.
COMPLICATION due to therapy
• Antifactor VIII antibody develops
• Virus transmission Hepatitis A-B-C-D + HIV
32. DISSAMINATED INTRAVASCULAR
COAGULATION
• DIC is condition characterized by thrombosis
within circulation.
• DIC can be induced by different mechanisms.
• Due to Endothelial cell damage by endotoxins in
G –ve septicemia results in tissue factor release
which in turn leads to coagulation cascade
activation through extrinsic pathway.
• The presence thromboplastin from damaged
tissue, placenta & fat embolus (following brain
injury & Fractures) may activate coagulation
• This results in excessive consumption of platelets
and coagulation factors, with secondary activation
of fibrinolysis leading to bleeding tendency.
33. DIC:
CAUSES
Infectious:
• E Coli
• Nessieria meningitis
• Strep pneumonia
• Malaria
Cancer
• Lung,Pancreas,
• Prostate
CLINICAL FEATURES:
Bleeding &
thrombosis, bleeding is more
than thrombosis.
Subacute DIC:
Occurs primarily in cancerous
pts results in superficial +
deep venous thrombosis.
Other Manifestation:
High incidence of cardio
respiratory failure
35. Treatment of DIC
Rx. Underlying cause.
General Measures:
• Correction of dehydration
• Renal failure
• Acidosis and
• Shock
Replacement:
• Platelets transfusion if platelets counts below
10,000/l
• cryoprecipitate to maintain plasma fibrinogen
level above 150 mg/dl
• FFP
• Heparin, if there is DVT, Pulmonarythrombosis.
36. Approach to a child with bleeding disorder
Bleeding
Not sick sick
Superficial bleeds Deep Bleeds
CBC, BT Factor
assay, Gene
analysis
Bone marrow
Blood culture CBC, Bonemarrow
LFT
RFT
FDP