

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Nrclinonc.2012.1
Semelhante a Nrclinonc.2012.1 (20)
Mais de Elsa von Licy
Mais de Elsa von Licy (20)
Nrclinonc.2012.1
- 1. REVIEWS Reactivation of hepatitis B virus and hepatitis C virus in patients with cancer Harrys A. Torres and Marta Davila Abstract | Infections with hepatitis B virus (HBV) or hepatitis C virus (HCV) are associated with significant morbidity and mortality among patients with cancer, especially in patients with hematologic malignancies and those who undergo hematopoietic stem-cell transplantation. Reported rates of HBV reactivation in HBV carriers who undergo chemotherapy range from 14–72%. In these patients, mortality rates range from 5–52%. HCV reactivation seems to be less common than HBV reactivation and is usually associated with a good outcome and low mortality. However, once severe hepatitis develops, as a result of viral reactivation, mortality rates seem to be similar among patients infected with HBV or HCV. Liver damage owing to viral reactivation frequently leads to modifications or interruptions of chemotherapy, which can negatively affect patients’ clinical outcome. Risk factors for the development of severe HBV or HCV reactivation need to be better defined to permit identification of patients who may benefit from preventive measures, early diagnosis, and therapy. In this article, we review the epidemiology, pathogenesis, risk factors, and clinical and laboratory manifestations associated with reactivation of HBV and HCV during immunosuppressive therapy. We also discuss strategies for the prevention and treatment of viral reactivation, including the management of reactivation with new antiviral agents. H. A. Torres, & M. Davila Nat. Rev. Clin. Oncol. 9, 156–166 (2012); published online 24 January 2012; doi:10.1038/nrclinonc.2012.1 Introduction Department of Infectious Diseases, Infection Control and Employee Health, Unit 1460 (H. A. Torres), Department of Gastroenterology, Hepatology and Nutrition, Unit 1466 (M. Davila), The University of Texas MD Anderson Cancer Center, 1515 Holcombe Boulevard, Houston, Texas 77030, USA. Correspondence to: H. A. Torres htorres@ mdanderson.org Viral infections are common and associated with signifi cant morbidity and mortality in patients with cancer, especially in patients with hematologic malignancies and in those who undergo hematopoietic stem-cell trans plantation (SCT). The impaired immunity associated with the underlying malignancy or the chemotherapyinduced immunosuppression predispose these patients to the development of new infections or reactivations of common viruses, including herpes simplex virus, varicella-zoster virus, cytomegalovirus, respiratory syn cytial virus, influenza virus, parainfluenza virus among others.1 Among the major viral infections observed in cancer patients and SCT recipients are hepatitis B virus (HBV) infection and hepatitis C virus (HCV) infection. Similarities and differences between these two viral infec tions are shown in Table 1 and Box 1. In this article, we review the epidemiology, pathogenesis, risk factors, and clinical and laboratory manifestations associated with the reactivation of HBV and HCV during immunosuppressive therapy, and discuss strategies for the prevention and treatment of viral reactivation. Reactivation of HBV infection Reactivation of HBV is a well-known complication in patients with cancer who undergo cytotoxic chemo therapy or other forms of immunosuppressive therapy. Competing interests H. A. Torres declares associations with the following companies: Astellas, Merck, Vertex. See the article online for full details of the relationships. M. Davila declares no competing interests. 156 | MARCH 2012 | VOLUME 9 Although HBV reactivation has been reported mostly in patients who tested positive for the hepatitis B surface antigen (HBsAg), viral reactivation can also occur in previously infected patients in whom the virus has appar ently been cleared. Such patients can be identified by the presence of antibodies against hepatitis B core antigen (anti-HBc) or against HBsAg (anti-HBs).2,3 Rates of HBV reactivation in HBV carriers who undergo chemotherapy vary, with reported values ranging from 14–72%. 2,4 Possible explanations for this wide variation include dif ferences in patient populations, types of tumors, chemo therapy regimens, definitions of reactivation, and study designs. Whereas some patients with HBV reactiva tion are asymptomatic, others have classic symptoms of hepatitis, including fatigue, anorexia, jaundice, ascites, and coagulopathy. Reactivation can also lead to hepatic encephalopathy, liver failure, and death. The disruption of anticancer treatment as a result of HBV reactivation can decrease overall survival.2,5 Mortality associated with HBV reactivation ranges from 5–52%.6–8 Diagnosis Definitions of HBV reactivation vary among investi gators. However, most scientists define HBV reactivation using one of the following three definitions: the develop ment of hepatitis in association with an increase in serum HBV DNA level to more than 1 log10 copies/ml higher than the level before therapy was initiated; an absolute increase in HBV DNA level exceeding 6 log10 copies/ml; or conversion of serum HBV-DNA-test results from negative to positive.9 Investigators also differ in their www.nature.com/nrclinonc © 2012 Macmillan Publishers Limited. All rights reserved
- 2. REVIEWS definitions of acute hepatitis. For study purposes, some researchers have defined acute exacerbation of chronic hepatitis as a more than threefold increase in serum levels of the enzyme alanine aminotransferase (ALT) between two consecutive determinations made at least 5 days apart.9 In the evaluation of patients with possi ble HBV reactivation, it is important to rule out other causes of hepatitis, including superinfection with other viruses (for example, hepatitis A virus, hepatitis D virus, cytomegalovirus, herpes simplex virus, varicella-zoster virus, Epstein–Barr virus, or adenovirus), chemotherapy- induced or drug-induced liver injury, sinusoidal obstruc tion syndrome, graft-versus-host disease, and the presence of tumor cells in the liver. Pathogenesis and clinical manifestations Stages of reactivation HBV reactivation as a result of cytotoxic chemo herapy t can generally be divided into three distinct stages (Figure 1). 10–12 Reactivation typically starts with an increase in viral replication caused by chemotherapyinduced immune suppression. The degree of increase in viral replication can be estimated by the magnitude of the rise in HBV DNA levels in serum. This rise can precede an elevation of ALT levels by up to 3 weeks. The first stage of increased viral replication can also feature re ppearance of hepatitis B e antigen (HBeAg) a and HBsAg, as well as a decrease in anti-HBs antibody titers. In the second stage of reactivation, functionality of the immune system is restored after chemotherapy is discontinued, and hepatocytes infected with HBV are destroyed. This stage can also involve an increase in ALT Key points ■■ Patients with cancer who are at risk of infection with hepatitis B virus (HBV) or hepatitis C virus (HCV) should undergo standard viral screening before initiation of cancer therapy ■■ HBV-DNA levels and HCV-RNA levels should be measured in patients who are at high risk of viral reactivation ■■ A substantial proportion of cancer patients with HBV or HCV infection develop liver dysfunction during chemotherapy, which often leads to discontinuation of potentially life-saving chemotherapy ■■ Treatment with antiviral agents can effectively prevent HBV reactivation, should be initiated before cancer therapy, and maintained during as well as for 6–12 months after discontinuation of immunosuppressive therapy ■■ HCV reactivation seems to be less frequent and less severe than HBV reactivation, but if severe hepatitis develops, mortality rates seem to be similar to those of HBV-infected patients ■■ Treatment of HCV reactivation is mainly supportive and new agents for the treatment of patients with HCV reactivation are urgently needed levels and the appearance of jaundice owing to hepato cellular injury. Furthermore, HBV DNA levels may decrease. The third stage of reactivation is the recovery phase, during which clinical hepatitis resolves and HBV markers return to baseline levels.10,12 The general pattern of HBV reactivation delineated by these three stages is not experienced by all patients, as specific patterns of reactivation can vary. In some patients, HBV DNA levels remain elevated but acute hepatitis does not develop owing to the lack of immune reconstitution. Occasionally, the second stage is more severe and can even be lethal. Other patients do not have a recovery stage, and may experience chronic hepatitis and deterioration of liver function.13 Table 1 | Basic differences between HBV and HCV24,99,100,101 Feature HBV HCV Size of virus 42 nm 40–70 nm Type of virus DNA virus of the Hepadnaviridae family RNA virus of the Hepacivirus genus within the Flaviviridae family Integration into the host genome Yes No Prevalence of infection Approximately 350 million people with chronic infections worldwide; an estimated 620,000 people die from HBV-related liver disease each year An estimated 180 million people are infected worldwide; HCV infection is the principal cause of death from liver disease and the leading indication for liver transplantation in the USA Geographic distribution Endemicity of HBV infection is high in some geographic areas, such as, south-east Asia and Sub-Saharan Africa Highest prevalence in north Africa (for example, Egypt) and south Asia. Most common genotypes (1–3) have a worldwide distribution Serologic pattern of infection Varied and complex The diagnosis generally requires testing of sera for antibodies to anti-HCV and HCV RNA Antigens or antibodies associated with infection HBsAg, HBcAg, HBeAg, anti-HBs, anti-HBc, anti-HBe Anti-HCV Duration of therapy Several serologic end points of antiviral therapy are used but optimal duration of therapy has not been established Standardized duration of therapy for the most-common viral genotypes Vaccination Available and highly effective in preventing infection HCV heterogeneity hinders the development of vaccines Post-exposure prophylaxis (immunoglobulin, vaccine) Available and effective Not available Abbreviations: HBcAg, hepatitis B core antigen; HBV, hepatitis B virus; HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus. NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | MARCH 2012 | 157 © 2012 Macmillan Publishers Limited. All rights reserved
- 3. REVIEWS Box 1 | Similarities between HBV, HCV, and associated disease24,99,100 ■■ ■■ ■■ ■■ ■■ ■■ ■■ ■■ ■■ ■■ ■■ ■■ Worldwide distribution Liver is the primary site of viral replication Both viruses can cause either acute or chronic hepatitis Patients with chronic infection can remain asymptomatic for years and, being unaware of their infections, are at risk of infecting others The differentiation between acute and chronic hepatitis depends mainly on the clinical presentation PCR-based diagnostic assays are available for the detection of nucleic acid levels Chronic infection is responsible for the majority of cases of viral-related morbidity and mortality, with liver failure, cirrhosis, and liver cancer as common causes of death Antiviral agents are available to treat chronic infection All patients with chronic infection should receive monitoring to assess progression of liver disease, development of hepatocellular carcinoma, and need for treatment Immunosuppressed patients (for example, those with HIV-coinfection or who are on hemodialysis) are at increased risk of infection Patients with chronic infection who initiate cytotoxic or immunosuppressive therapy (for example, patients with cancer, or recipients of organ or stem-cell transplants) are at risk for viral reactivation No standard definition of viral reactivation exists Risk factors The risk of HBV reactivation is influenced by both the type of malignancy and the particular immuno suppressive therapy that is administered. Most patients in whom HBV is reactivated have hematologic malig nancies. Patients with lymphoma may be at particular risk.14,15 Nonetheless, an increasing number of cases have been described among patients with solid tumors, among whom the highest rates of HBV reactivation have been reported for patients with breast cancer (as high as 41–56%).16,17 HBV reactivation has also been observed in up to 36% of patients with hepatocellular carcinoma who received systemic chemotherapy.18 High rates of reactiva tion and substantial exacerbation of HBV in patients with HBV-related hepatocellular carcinoma who were under going transarterial chemoembolization (TACE) has been reported in one study,19 but not in another study.20 Other host and viral factors have also been identified as significant risk factors for HBV reactivation. One of the most important risk factors is a high serum HBV viral load.21 In a study of 137 patients who underwent autologous hematopoietic SCT, HBV reactivation was more common among HBsAg-positive patients with detectable serum HBV DNA before transplantation than among patients in whom no HBV DNA was detected.21 Furthermore, a high HBV DNA level (105 copies/ml) was the most-important risk factor for HBV reacti vation.21 Other risk factors include male sex, young age (mean age 44 years, range 20–64 years), HBeAg seropositivity, use of corticosteroids or use of certain chemothera eutic agents, including anthracyclines, p cyclophosphamide, and vinca alkaloids. 2,14,15 Use of monoclonal antibodies (such as rituximab8 and alem tuzumab22) alone or in combination with other agents has also been linked to HBV reactivation. Accounting for 39% of the reported cases, HBV reactivation was the most frequent viral infection in patients treated with rituximab and associated with a 52% mortality rate 158 | MARCH 2012 | VOLUME 9 owing to liver failure.8 Furthermore, HBV reactivation was observed among rituximab-treated patients who were HBsAg-negative but anti-HBc positive.23 Prevention and treatment Screening Preventing HBV reactivation might be superior to inter vention after reactivation has already occurred. The first step in prevention should be screening for HBV markers before initiation of chemotherapy in patients who are at increased risk of viral reactivation. These include patients who were born in regions of intermediate and high HBV endemicity (HBsAg prevalence ≥2%), children of indivi duals who were born in regions with high HBV endemi city (HBsAg prevalence ≥8%), patients with a history of intravenous drug use, patients undergoing hemo dialysis, HIV-positive patients, and men who have sex with men.24 Since physicians may not accurately identify individuals who are at high risk of HBV infection, one could make a case that all patients who are scheduled to receive immuno uppressive therapy should be screened s for HBV given the substantial consequences of reacti vation. Indeed, such routine testing was recommended by the US Centers for Disease Control and Prevention (CDC) in 2008.24 This recommendation prompted ASCO to develop a provisional clinical opinion on the subject of HBV screening, which was published in 2010.25 ASCO stated that insufficient evidence exists to determine the net benefits and harms of routine screening for chronic HBV infection in patients with cancer who are about to receive immunosuppressive therapy or who are already receiving such therapy. Physicians are advised to con sider screening of high-risk patients or those in whom highly immuno uppressive therapy is planned, includ s ing (but not limited to) patients undergoing hemato poietic SCT or who are treated with drug regimens that include rituximab.25 If screening is undertaken, it should include testing for the presence of HBsAg and anti-HBc (Figure 2). Patients who are HBsAg-positive should be tested for HBeAg, antibodies against HBeAg (anti-HBe), and levels of HBV DNA should be determined. Patients who are HBsAgnegative but anti-HBc-positive should be tested for antiHBs antibodies. Patients who are negative for anti-HBs antibodies have not developed immunity against HBV, and HBV-DNA testing should be the next step to rule out an occult HBV infection. Use of antiviral drugs Prophylaxis against HBV reactivation should be initiated as early as possible before the onset of immunosuppres sive therapy in HBsAg-positive patients.5,7,11 In patients with high HBV DNA levels (2,000 inter ational units n [IU]/ml) and elevated ALT levels, therapy should be ini tiated immediately with the aim of lowering viral rep lication and disease activity as much as possible before chemotherapy is administered. Although five orally administered drugs are currently approved for the treatment of chronic HBV infection in the USA (lami vudine, telbivudine, adefovir, entecavir, and teno ovir), f www.nature.com/nrclinonc © 2012 Macmillan Publishers Limited. All rights reserved
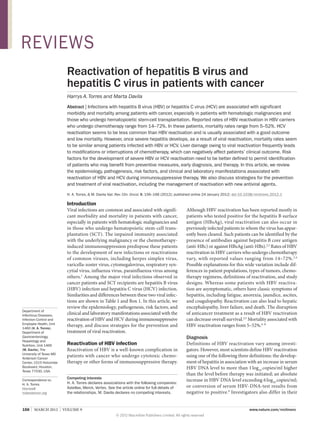
- 4. REVIEWS 1st stage 2nd stage 3rd stage Initiation of cytotoxic chemotherapy Discontinuation of cytotoxic chemotherapy Recovery of liver function Immunosuppresion Immune recovery Return to chronic viral replication level (baseline) Rapid viral replication in hepatocytes Rebound of the T-cell response T cells Hepatocytes Natural killer cells Increased inflammatory activity T cells Inhibition of cytokine production and cytotoxicity by HCV and possibly HBV Hepatocytes T cells Virus ALT levels Normal Increased, occasionally normal Normal Viral load Increased Decreased Decreased or return to baseline Figure 1 | The three stages in the pathogenesis of HBV and HCV reactivation. Reactivation of HBV or HCV as a result of chemotherapy can generally be divided into three stages. Reactivation typically starts with an increase in viral replication caused by chemotherapy-induced immune suppression (stage 1). After chemotherapy is discontinued, the function of the immune system is restored, and hepatocytes infected with HBV or HCV are destroyed (stage 2). In the recovery stage (stage 3), clinical hepatitis (indicated by an increase in ALT levels) resolves and markers of HBV or HCV infections return to baseline levels. Abbreviations: ALT, alanine aminotransferase; HBV, hepatitis B virus; HCV, hepatitis C virus. the published experience in 2011 on the prevention and treatment of HBV reactivation is mostly limited to lamivudine. Lamivudine has proven efficacy in the prevention of HBV reactivation in patients with hematologic malig nancies and in patients with solid tumors, and has an excellent safety profile. In one study, 30 patients with lymphoma who were positive for HBsAg were randomly assigned to receive lamivudine 100 mg daily 1 week before initiation of chemotherapy or only when serologic evidence of HBV reactivation was observed. None of the patients in the prophylactic-therapy group experienced HBV reactivation, as opposed to eight patients (53%) in the deferred-treatment group (P = 0.002).26 In another randomized study in which 43 HBsAg-positive patients with non-Hodgkin lymphoma were randomly assigned to receive prophylactic lamivudine either on day 1 of chemo herapy or not until they had shown an increase t in ALT levels, patients in the prophylactic-therapy group had a significantly lower risk of HBV reactivation than patients who were withheld lamivudine initially (11.5% versus 56%; P = 0.001).27 The efficacy of preventive lamivudine was addressed in a meta-analysis of 14 studies, which included 275 patients who received lamivudine and 475 control partici ants.28 p The investigators found that preventive treatment with lamivudine was associated with a relative risk of 0.00–0.21 for HBV reactivation and HBV-related hepatitis.28 Despite differences in their design, all studies showed beneficial effects of preventive lamivudine, with the exception of one study in which one HBV-related death was noted.28 In another meta-analysis, which included nine studies and a total of 396 participants, the cumulative prevalence of HBV reactivation was 8.6% (11 of 127 patients) in the prophylaxis group versus 50.6% (136 of 269 patients) in the control group. Again, lamivudine prophylaxis signifi cantly reduced HBV reactivation, and a trend towards a reduction in HBV-associated mortality was observed.29 When to start or discontinue anti-HBV treatment for prevention of HBV reactivation is an area of uncertainty. NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | MARCH 2012 | 159 © 2012 Macmillan Publishers Limited. All rights reserved
- 5. REVIEWS HBsAg-positive HBsAg-negative Anti-HBc-positive Check HBV DNA Anti-HBs-positive Conventional chemotherapy Monoclonal antibody therapy or stem-cell transplantation Use lamivudine Prophylaxis recommended for at least 6 months after discontinuation of all immunosuppressive therapy Use entecavir or tenofovir Prophylaxis recommended for 12 months or more after discontinuation of immunosuppressive therapy Use entecavir or tenofovir Patients should be on treatment until they reach end points as in immunocompetent patients No treatment needed Check HBV DNA HBV DNA-positive HBV DNA 2,000 IU/ml (2) HBV DNA 2,000 IU/ml (1) Anti-HBs-negative HBV DNA-negative Start antiviral therapy according to HBV DNA level (1) or (2) Consider HBV vaccination Figure 2 | Algorithm for the management of patients with possible HBV infection who undergo immunosuppressive therapy. Patients with cancer should be screened for HBV infection by testing them for the presence of HBsAg, and antibodies against HBc or the HBsAg. Patients who are HBsAg-positive or who are anti-HBc positive but HBsAg-negative or anti-HBs-negative, should have HBV DNA levels measured to guide future management. An individualized approach with careful monitoring of ALT levels and HBV DNA levels is recommended if chemotherapy or other immunosuppressive therapy is initiated. Abbreviations: HBc, hepatitis B core antigen; HBV, hepatitis B virus; HBsAg, hepatitis B surface antigen; IU, international units. For HBsAg-positive patients receiving conventional chemo herapy, lamivudine was recommended to be t administered for at least 6 months after discontinua tion of all immunosuppressive therapy.7,10,11,30 Patients who receive therapies with monoclonal antibodies or undergo hematopoietic SCT may need to take lamivudine for 12 months or more.31–33 Should HBV be reactivated in a patient who has not received prophylactic anti-HBV therapy, antiviral treatment must be instituted immedi ately and all chemotherapy must be suspended. However, rates of mortality from hepatic failure may still be high even when lamivudine is administered.7,32 Patients with high baseline HBV DNA levels (2,000 IU/ml) should continue lamivudine treatment until they reach clinical treatment end points, as is the practice in immunocompetent patients who receive anti viral treatment.30 These end points include normaliza tion of serum ALT levels, decrease in serum HBV DNA to undetectable levels, loss of HBeAg (with or without detection of anti-HBe), and improvement in liver histo logy.30 Over the course of lamivudine therapy, mutations in the YMDD motif of the HBV DNA-polymerase gene can develop, which confer resistance to lamivudine.7 In immunocompetent patients with chronic HBV infec tion, the cumulative rate of resistance to lamivudine is reported to be 24% after 1 year of treatment, and 65–70% after 5 years of treatment.34 For patients who need prolonged anti-HBV therapy (over 12 months), it is appropriate to avoid lamivudine and to use instead drugs associated with a low incidence of resistance, such as entecavir or tenofovir, as first-line anti-HBV therapy.30,35 HBsAg-negative but anti-HBc-positive patients The precise incidence of reactivation in patients who are HBsAg-negative but anti-HBc-positive is unknown. 160 | MARCH 2012 | VOLUME 9 Various studies have suggested a low risk of reactiva tion in this group (2%).2,32 However, the risk might be much higher if such patients receive rituximab (2.7– 45%). 36 Reactivation of HBV infection in anti-HBspositive patients can also occur, a phenomenon known as ‘reverse seroconversion’. In patients who have undergone allo eneic hematopoietic SCT, the rate of reverse sero g conversion has been reported to be as high as 40% after 2 years and 70% after 5 years.37 Patients who are HBsAg-negative but anti-HBc- positive should undergo further testing for HBV DNA to rule out an occult infection. Patients who are HBVDNA-positive should be considered for antiviral pro phylaxis, especially if they might undergo prolonged immunosuppression or SCT. 10 Alternatively, such patients can be followed closely by performing serial HBV DNA tests, although this approach has not been thoroughly evaluated in clinical studies (Figure 2). In our own practice, we favor prophylactic therapy in patients who are HBV-DNA-positive. If the patient refuses pro phylactic treatment, we offer monthly serum HBV DNA testing during therapy and for 6 months after comple tion of therapy. Well-designed clinical trials are needed to investigate the efficacy and safety of early diagnosis of reactivation by HBV DNA monitoring in patients who are HBsAg-negative and anti-HBc-positive and/or anti-HBs-positive. Reactivation of HCV infection In patients with cancer, HCV infection is more common than HBV infection, even in geographic areas where HBV infection is endemic.38,39 However, HCV reactiva tion following immunosuppressive therapy is rare.15,38–41 For instance, in an Italian study of 98 patients with B‑cell non-Hodgkin lymphoma, three of eight (38%) www.nature.com/nrclinonc © 2012 Macmillan Publishers Limited. All rights reserved
- 6. REVIEWS HBsAg-positive patients experienced HBV reactivation after chemo herapy, but none of the 11 patients with t anti-HCV antibodies experienced HCV reactiva ion.42 t In another study of patients with B‑cell non-Hodgkin lymphoma, the incidence of acute exacerbation of hepa titis (indicated by an ALT increase) was higher among patients with chronic HCV infection than in HCVuninfected patients (26.3% versus 2.1%),43 suggesting that HCV reactivation occurred and can cause clinically relevant complications. Although HCV reactivation seems to be more common in patients with hematologic malignancies,38,44 it has also been reported in patients with solid tumors45,46 and in patients who have undergone SCT.47,48 At present, no reliable methods to predict an individual’s risk of HCV reactivation exist. The health consequences of HCV reactivation seem to be less severe than those of HBV reactivation.49,50 Only a few deaths related to HCV reactivation have been reported.51 However, if severe hepatitis secondary to viral reactivation develops, mortality rates of HBV-infected and of HCV-infected patients seem to be similar.52–54 In the absence of severe hepatitis, the likelihood of a fatal outcome of HCV reactivation is somewhat unpredictable.55 Diagnosis Studies of HCV reactivation are hard to compare directly as definitions for HCV reactivation vary. We and others39,50 have defined HCV reactivation as an at least threefold increase in serum ALT level in a patient in whom the tumor has not infiltrated the liver, who did not receive hepatotoxic drugs and who had no recent blood transfusions or other systemic infections besides HCV. Changes in liver enzyme levels can be accompanied by reappearance of HCV RNA or a sudden increase in the serum HCV RNA level.39 Whether immunosuppressive therapy leads to HCV reactivation in patients with cancer in whom the infec tion has cleared either spontaneously or secondary to therapy is uncertain. When HCV RNA clearance is achieved either spontaneously or in response to anti viral therapy in recipients of solid organ transplants, no relapse is observed in plasma, liver, or peripheral blood mononuclear cells during chronic immuno uppressive s treatment with agents such as calcineurin inhibi tors, cortico teroids, antimetabolites, anti-thymocyte s globulins, or anti-IL‑2-receptor blockers. This find ing suggests the complete and permanent cure of HCV infection resulting from the elimination of HCV before transplantation.56 Chronically infected patients have stable HCV RNA levels that may vary by approximately 0.5 log10 IU/ml.57 Therefore, an increase in HCV viral load of more than 1 log10 IU/ml may be a sign of HCV reactivation. However, more studies are needed to better define the relationship between changes in HCV viral load and liver function during chemotherapy.58 HCV infection is diagnosed using serologic assays for antibodies and molecular tests for viral parti les. c However, patients with cancer, especially those with hematologic malignancies, can have false-negative antibody results. 59–62 Thus, in patients infected with HCV in whom HCV reactivation is suspected during chemo herapy, HCV RNA levels should be measured to t confirm reactivation. Pathogenesis and clinical manifestations HBV and HCV reactivation seem to be mediated by similar pathogenetic mechanisms. 41,63–65 As for HBV reactivation,39,66 reactivation of HCV infection occurs when chemotherapy-induced immunosuppression facili tates HCV replication by reducing the immune response that controls viral infections (Figure 1).65 In addition, when the administration of cytotoxic chemotherapy or immuno uppressive drugs is suspended in patients s with chronic HCV infection the period of depressed cel lular immunity can be followed by an ‘immunological rebound’. This phenomenon is characterized by resto ration of immune function and increased inflamma tory activity in the liver, resulting in rapid destruction of the HCV-infected hepato ytes and liver injury.44,65 c Some subgroups of cancer patients that seem to have an elevated risk for HCV reactivation include males and patients with lymphoma (mainly non-Hodgkin lym phoma), lymphopenia, or use of corticosteroids as part of anticancer treatment.44,50,51 Reactivation after specific treatments Corticosteroids have traditionally been associated with cases of HCV reactivation.51,67 Several pathogenic mechanisms have been postulated, including enhanced HCV infectivity owing to upregulated expression of viral receptors on the surface of the hepatic cells (which facilitates virus entry into hepatocytes), 68 increased replication of HCV in vitro (noted in peripheral blood mononuclear cells that were cultivated in the presence of corticosteroids),69 and enhanced viral replication in vivo (observed in liver-allograft recipients after the injection of a high dose of corticosteroids).69 HCV reactivation has been associated with several immunosuppressive and chemotherapeutic agents, including alemtuzumab, bleomycin, busulfan, cisplatin, cyclophosphamide, cyclosporine, cytarabine, dacarba zine, doxorubicin, etoposide, gemcitabine, methotrexate, vinblastine, and vincristine. 45,47,48,51,58,70–73 However, many patients with HCV reactivation during treatment with one of these drugs were simultaneously treated with corticosteroids.48,70,72,74 We found that administration of systemic corticosteroids was linked to HCV reactiva tion75 but was not associated with acute exacerbation of chronic HCV infection.73 Whether corticosteroid therapy alone or in combination with other agents leads to reac tivation of HCV infection and acute exacerbation of chronic HCV infection remains to be determined. A possible relationship between rituximab and HCV reactivation in patients with cancer has been reported,70,74,76 but whether rituximab has an adverse effect on the natural history of HCV infection and its complications is unclear. 77 Some studies suggest that rituximab is not associated with HCV reactivation. In NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | MARCH 2012 | 161 © 2012 Macmillan Publishers Limited. All rights reserved
- 7. REVIEWS a case series of HCV-infected patients with lymphoma who received a rituximab-based regimen, chemotherapy was changed as a result of HCV reactivation in only one of nine patients, and none of the patients developed hepatic failure.78 Moreover, rituximab is increasingly being used for the treatment of HCV-associated cryo globulinemic vasculitis, and data from short-term use of rituximab in this setting indicate a favorable clinical response with only mild elevation of HCV RNA levels (to approximately twice the baseline levels), no substantial changes in serum transaminase levels, and no deteriora tion of liver disease.79 Whether the likelihood of HCV reactivation differs between patients receiving rituximab because of HCV-related vasculitis and those receiving the drug for the treatment of conditions unrelated to HCV remains unknown. Other studies, however, indicate that rituximab is associated with HCV reactivation. We recently analyzed 308 HCV-infected patients with a variety of cancer types who were treated with various regimens tailored to their underlying malignancy.75,80 Interestingly, only the administration of rituximab-containing chemo herapy t was associated with both acute exacerbation80 and reacti vation75 of chronic HCV infection. In a recently pub lished series from Italy that included eight HCV-infected patients (five with B‑cell non-Hodgkin lymphoma and three with chronic lymphocytic leukemia), all seven patients who underwent rituximab-based chemo therapy had an increase in the plasma HCV load of at least 1.5 log10 IU/ml (median 2.2; range 1.5–2.6 IU/ml).81 Whether HCV reactivation is related to high cumula tive doses of rituximab, as observed for HBV reactiva tion, remains uncertain.73 Evidence of a lack of HCV reactivation in patients receiving chemotherapy not including rituximab has been reported in three studies of patients with non-Hodgkin lymphoma.42,43,81 Given the association between rituximab and HBV reactiva tion, a hypo hetical association between rituximab t and HCV reactivation ought to be examined with well-designed studies.8 In HCV-infected patients without active hepatitis, findings of the majority of studies suggest that inhibi tors of tumor necrosis factor (such as infliximab) are either bene icial or, at least, not detrimental.82,83 No case f of HCV reactivation associated with the use of these agents has been reported. Studying 84 patients with HCV-associated hepato cellular carcinoma treated with TACE, we compared HCV RNA levels before and after TACE in three patients from whom such samples were available and who under went a total of six TACE procedures. Six episodes of acute exacerba ion of hepatitis were noted—one after t each TACE procedure. No signs of HCV reactivation (1 log10 IU/ml increase in HCV RNA levels from base line) were identified in the three patients.84 Larger pro spective series are warranted to better define the risk of HCV reactivation after TACE. Patients with HCV infection who undergo SCT can experience severe hepatic dysfunction and ful minant hepatic failure. HCV RNA levels can increase 162 | MARCH 2012 | VOLUME 9 substantially during immunosuppressive therapy —which usually includes cyclosporine, prednisone, or both—and fulminant hepatitis can develop when immuno uppressive drugs are withdrawn. 47,48,85,86 In s a large Italian study of 57 HCV-infected patients who underwent SCT, the risk of reactivation after transplan tation was significantly lower if patients underwent autologous SCT rather than allogeneic SCT (16% versus 100%, P = 0.004). In the allogeneic SCT group, reactiva tion occurred mainly within 6 months after SCT, whereas in the autologous SCT group, reactivation predominantly occurred within the first 3 months.53 In a Japanese multi center study of 135 patients with HBV or HCV infection who received allo eneic transplants, transient hepati g tis was more common in HBV-infected patients than in HCV-infected patients, but the rates of fulminant hepatitis and death due to hepatic failure were similar in both groups.54 However, these data should be analyzed with caution as they were obtained retrospectively and without consideration of other factors associated with liver dysfunction (such as co-infections with pathogens other than HBV or HCV, or use of hepatotoxic drugs) or viral loads. Timing of reactivation The timing of HCV reactivation in relation to the administration of chemotherapeutic drugs varies. Acute exacerbation of HCV infection (indicated by an ALT increase) can occur during chemotherapy, but is usually observed weeks or months after chemotherapy, corti costeroids, or after both have been withdrawn.44,49,50,60 Among 18 patients with hematologic malignancies and acute exacerbation of chronic HCV infection, the increase in ALT levels was first noted at a mean of 19 days (range 14–32 days) after withdrawal of chemo therapy (mostly after the fourth or fifth cycle).49 In our recent study that included 19 patients with acute exac erbation of HCV infection after initiation of rituximab, the time to onset of hepatitis flare was 30 days (median; range 1–200 days) after discontinuation of rituximab.75 Among HCV-infected patients who experienced severe liver dysfunction during chemotherapy, liver function tests returned to normal within 2–3 weeks after the caus ative agent was discontinued.49 However, in patients with fulminant hepatitis, peak ALT levels above 6,000 IU/l and recovery times of about 7 weeks have been reported.51 In most patients with HCV reactivation, acute eleva tion of ALT levels or HCV RNA levels causes no symp toms, and ALT elevations are mild and transient. In some studies, the increase in ALT can be preceded by an increase in HCV RNA levels.81 For instance, in a recent study of eight patients with hematologic malignancies, HCV reactivation was followed by an increase in ALT serum values 3–5 months after rituximab-based chemo therapy was discontinued.81 The possibility that patients were evaluated at the different stages of HCV reactiva tion (Figure 1) could explain the lack of simultaneous elevation of HCV viral load and ALT levels in some cases. The diagnosis of HCV reactivation can be further compli ated because low HCV RNA levels are c www.nature.com/nrclinonc © 2012 Macmillan Publishers Limited. All rights reserved
- 8. REVIEWS Anti-HCV-positive before initiation of immunosuppressive therapy* Measure baseline HCV RNA and ALT levels If indicated, start chemotherapy or immunosuppressant monitoring ALT every 1–2 weeks and HCV RNA every 4 weeks (until 3 months after treatment withdrawal of each cycle) Normal ALT level Raised ALT level† At least 1 log IU/ml increase in HCV RNA level compared to baseline HCV RNA viral load Continue monitoring Check HCV RNA levels every 2–4 weeks while monitoring ALT. If at least 1 log IU/ml increase in HCV RNA level compared with baseline HCV RNA viral load Consider discontinuation of chemotherapy or other immunosuppressive therapy only if increasing ALT level precludes their use Figure 3 | Approach to management of HCV-positive patients with cancer who undergo chemotherapy or immunosuppressive therapy. Patients with cancer should be screened for HCV infection with serologic assays that detect specific antibodies against HCV (anti-HCV). In patients with anti-HCV antibodies, an HCV RNA assay is recommended for diagnosis. An individualized approach with careful monitoring of ALT and HCV RNA levels is recommended if chemotherapy or other immunosuppressive therapy is initiated. *Or HCV RNA level in high-risk patients (for example, patients with nonHodgkin lymphoma and unexplained liver disease). ‡Defined as an at least threefold increase from baseline. Abbreviations: ALT, alanine aminotransferase; HCV, hepatitis C virus. occasi nally observed in cases of severe acute exacerba o tion, possibly because of the absence of suitable cells for viral replication secondary to massive liver-cell necrosis.51 Occurrence of severe hepatic dysfunction Few studies have compared the development of severe hepatic dysfunction between HCV-infected patients and those not infected with HCV. In a study of patients with acute myelogenous leukemia, ALT serum levels were higher in HCV-infected patients than in patients who were not infected with HCV.87 Data from one study demonstrated that the incidence of severe hepatic dys function during or after chemotherapy was higher in HCV-infected patients than in HCV-negative patients.88 However, in a study of 33 HCV-positive patients with hematologic malignancies who received intermittent chemotherapy, severe flare of hepatitis occurred in only two patients.49 Findings from noncomparative studies indicate that some HCV-positive patients may have severe exacer bation of HCV infection resulting in necrosis, hepatic failure, and death.51,58,72 Besson and colleagues, demon strated that up to 65% of patients with chronic HCV infection developed significant liver dysfunction during chemotherapy against diffuse large B‑cell lymphoma, and that almost half of the patients with liver dysfunc tion had grade 3–4 hepatic dysfunction.89 The proportion of HCV-positive patients with hepatic dysfunction and the severity of dysfunction tended to increase with the number of chemotherapy courses.89 In some cases of fatal fulminant hepatitis, HCV RNA levels increased dramati cally during treatment, and a sharp decrease in HCV RNA levels together with a marked increase in ALT levels were observed when chemotherapy was withdrawn.51 Prevention No drugs are currently approved for the prevention of HCV reactivation in patients with HCV infection who undergo chemotherapy. The risk of HCV reactivation in such patients might be reduced by using lower doses of immunosuppressive drugs, close monitoring of ALT levels (especially after chemotherapy is reduced or with drawn), and by measuring HCV RNA levels early during episodes of potential viral reactivation. Given the pos sibility of immune-mediated hepatocyte injury upon HCV reactivation, some researchers have speculated that gradual tapering of immunosuppressants could be another strategy to prevent HCV reactivation.51,85,90 However, as it is unknown which patients with chronic HCV infection are at risk of reactivation after cessation of immunosuppressive treatment, caution is advised with respect to this intervention, which has not been formally tested and could negatively affect patients’ response to cancer therapy without preventing HCV reactivation. Implications for chemotherapy An approach to the management of HCV-positive patients with cancer who are undergoing chemo herapy t or other immunosuppressive therapy is shown in Figure 3. Chemotherapy can generally be administered in selected patients with HCV infection if they are monitored for viral reactivation during therapy.55 Several studies have shown that hepatic dysfunction can lead to frequent modifications or interruptions of chemotherapy in patients with HCV reactivation, wors ening their overall outcomes.45,49,60,78,89,91,92 In a series of 160 HCV-positive patients with non-Hodgkin lym phoma, eight patients (5%) did not complete the planned treatment and 15 patients (9%) had their treatment NATURE REVIEWS | CLINICAL ONCOLOGY VOLUME 9 | MARCH 2012 | 163 © 2012 Macmillan Publishers Limited. All rights reserved
- 9. REVIEWS postponed because of liver dysfunction.58 In that study, median progression-free survival was significantly shorter for patients who experienced liver dysfunction than for those who did not (2 years versus 3.7 years; P = 0.03).58 At our institution, chemotherapy was discon tinued in up to 45% of patients with acute exacerbation of HCV infection,80 but chemotherapy can usually be restarted once liver function returns to normal. Treatment What constitutes the best treatment for HCV reactiva tion is unclear, and, at present, treatment is mainly sup portive. Patients with chronic HCV infection are treated with the combination of pegylated interferon‑α and riba virin.93,94 The use of direct-acting antiviral drugs (such as the recently approved inhibitors of nonstructural protein 3/4A (NS3/4A) protease [boceprevir or telapre vir], or NS5B polymerase inhibitors) has not been evalu ated in patients with cancer. Boceprevir and telaprevir can inhibit hepatic drug-metabolizing enzymes such as cytochrome P450 (CYP) 2C, CYP3A4, or CYP1A.95 Therefore, these agents potentially interact with various drugs that are co-administered in patients with cancer. These new antiviral drugs should be used with caution in patients with cancer and preferably should be prescribed only by clinicians with extensive experience in working with this patient population.96 Anti-HCV therapy has traditionally been avoided during chemotherapy in HCV-infected patients with cancer because the hematologic adverse effects of antiHCV drugs can exacerbate the toxicity of chemotherapy, which can involve complications such as severe cyto penias and potentially life-threatening infections. 91 Results of a small case series published in 2010 suggest that antiviral treatment can be considered when liver dysfunction prohibits the administration of life-saving chemotherapy.97 However, there is currently not enough information to recommend administering anti-HCV therapy concomitantly with standard chemotherapy even in patients with HCV reactivation. Large-scale studies are needed to better define which patients with cancer are most likely to benefit from simultaneous antiviral therapy and cytotoxic chemotherapy. Notably, antiviral treatment with pegylated interferon α and rib avirin should not be used early in the post- ransplant t period (2 years after transplantation) in patients who have undergone allogeneic SCT as interferon‑α 1. 2. 3. Torres, H. A., Boeckh, M. Chemaly, R. F. in Medical Care of Cancer Patients (eds Yeung, S. J., Escalante, C. Gagel, R. F.) 151–161 (B. C. Decker Inc Publisher, Shelton, CT, 2009). Lok, A. S. et al. Reactivation of hepatitis B virus replication in patients receiving cytotoxic therapy. Report of a prospective study. Gastroenterology 100, 182–188 (1991). Law, J. K. et al. Fatal reactivation of hepatitis B post-chemotherapy for lymphoma in a hepatitis B surface antigen-negative, hepatitis B core antibody-positive patient: potential implications for future prophylaxis recommendations. Leuk. Lymphoma 46, 1085–1089 (2005). 164 | MARCH 2012 | VOLUME 9 4. 5. 6. therapy might precipitate or induce the development of graft-versus-host disease.98 Conclusions Reactivation of HBV or HCV is associated with sub stantial morbidity and mortality in patients with cancer. Therefore, patients who require chemotherapy, SCT, or treatment with high-dose corticosteroids should rou tinely be screened for HBV and HCV before institution of immunosuppressive therapy with standard tests such as measurements of HBsAg, anti-HBc antibodies, and anti-HCV antibodies. Screening for serum HBV DNA and HCV RNA should also be performed in patients who are at high risk of viral hepatitis. In any patient with a history of chronic infection who develops liver dysfunction during or after chemotherapy, the possibility of HBV or HCV reactivation should be considered. Periodic monitoring (at least monthly) of ALT levels is recommended during chemotherapy and after chemotherapy is reduced or withdrawn. In patients with elevated ALT levels, levels of HBV DNA and HCV RNA should be measured to confirm viral reactivation. A substantial proportion of cancer patients with HBV or HCV infection—mainly those with nonHodgkin lymphoma—develop liver dysfunction during chemo herapy, which often leads to discontinuation of t potentially life-saving chemotherapy. Unlike HCV reactivation, HBV reactivation is a serious but preventable complication of immuno suppressive therapy. Prophylactic anti-HBV therapy with lamivudine is effective, and lamivudine has an excellent safety profile. For patients with high HBV DNA levels and for those who require prolonged therapy, the use of newer nucleoside or nucleotide analogs such as enteca vir or tenofovir is recommended. As treatment of HCV reactivation is currently mainly supportive, new agents to treat HCV reactivation are urgently needed. Review criteria Information for this Review was identified by searches of the PubMed database and of the extensive reference resources of the authors. The search terms included “hepatitis B virus”, “hepatitis C virus”, and “reactivation”. Abstracts and reports from meetings were included only when they related directly to subsequently published work. We reviewed all articles published in English between January 1970 and October 2011. Alexopoulos, C. G., Vaslamatzis, M. Hatzidimitriou, G. Prevalence of hepatitis B virus marker positivity and evolution of hepatitis B virus profile, during chemotherapy, in patients with solid tumours. Br. J. Cancer 81, 69–74 (1999). Yeo, W. et al. Lamivudine for the prevention of hepatitis B virus reactivation in hepatitis B s‑antigen seropositive cancer patients undergoing cytotoxic chemotherapy. J. Clin. Oncol. 22, 927–934 (2004). Liang, R., Lau, G. K. Kwong, Y. L. Chemotherapy and bone marrow transplantation for cancer patients who are also chronic hepatitis B carriers: a review of the problem. J. Clin. Oncol. 17, 394–398 (1999). 7. Lalazar, G., Rund, D. Shouval, D. Screening, prevention and treatment of viral hepatitis B reactivation in patients with haematological malignancies. Br. J. Haematol. 136, 699–712 (2007). 8. Aksoy, S. et al. Rituximab-related viral infections in lymphoma patients. Leuk. Lymphoma 48, 1307–1312 (2007). 9. Lau, G. K. Hepatitis B reactivation after chemotherapy: two decades of clinical research. Hepatol. Int. 2, 152–162 (2008). 10. Hoofnagle, J. H. Reactivation of hepatitis B. Hepatology 49 (Suppl. 5), S156–S165 (2009). 11. Mindikoglu, A. L., Regev, A. Schiff, E. R. Hepatitis B virus reactivation after cytotoxic www.nature.com/nrclinonc © 2012 Macmillan Publishers Limited. All rights reserved
- 10. REVIEWS 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. 24. 25. 26. 27. chemotherapy: the disease and its prevention. Clin. Gastroenterol. Hepatol. 4, 1076–1081 (2006). Xunrong, L., Yan, A. W., Liang, R. Lau, G. K. Hepatitis B virus (HBV) reactivation after cytotoxic or immunosuppressive therapy —pathogenesis and management. Rev. Med. Virol. 11, 287–299 (2001). Su, W. P et al. Long‑term hepatic consequences . of chemotherapy‑related HBV reactivation in lymphoma patients. World J. Gastroenterol. 11, 5283–5288 (2005). Yeo, W. et al. Comprehensive analysis of risk factors associating with Hepatitis B virus (HBV) reactivation in cancer patients undergoing cytotoxic chemotherapy. Br. J. Cancer 90, 1306–1311 (2004). Yeo, W. et al. Frequency of hepatitis B virus reactivation in cancer patients undergoing cytotoxic chemotherapy: a prospective study of 626 patients with identification of risk factors. J. Med. Virol. 62, 299–307 (2000). Yeo, W. et al. Hepatitis B virus reactivation in breast cancer patients receiving cytotoxic chemotherapy: a prospective study. J. Med. Virol. 70, 553–561 (2003). Dai, M. S., Wu, P Shyu, R. Y., Lu, J. J. . F., Chao, T. Y. Hepatitis B virus reactivation in breast cancer patients undergoing cytotoxic chemotherapy and the role of preemptive lamivudine administration. Liver Int. 24, 540–546 (2004). Yeo, W. et al. Hepatitis B reactivation in patients with hepatocellular carcinoma undergoing systemic chemotherapy. Ann. Oncol. 15, 1661–1666 (2004). Jang, J. W. et al. Transarterial chemo‑ lipiodolization can reactivate hepatitis B virus replication in patients with hepatocellular carcinoma. J. Hepatol. 41, 427–435 (2004). Park, J. W. et al. Risk of hepatitis B exacerbation is low after transcatheter arterial chemoembolization therapy for patients with HBV‑related hepatocellular carcinoma: report of a prospective study. Am. J. Gastroenterol. 100, 2194–2200 (2005). Lau, G. K. et al. High hepatitis B virus (HBV) DNA viral load as the most important risk factor for HBV reactivation in patients positive for HBV surface antigen undergoing autologous hematopoietic cell transplantation. Blood 99, 2324–2330 (2002). Iannitto, E. et al. Hepatitis B virus reactivation and alemtuzumab therapy. Eur. J. Haematol. 74, 254–258 (2005). Targhetta, C., Cabras, M. G., Mamusa, A. M., Mascia, G. Angelucci, E. Hepatitis B virus‑related liver disease in isolated anti‑hepatitis B‑core positive lymphoma patients receiving chemo- or chemo-immune therapy. Haematologica 93, 951–952 (2008). Weinbaum, C. M. et al. Recommendations for identification and public health management of persons with chronic hepatitis B virus infection. MMWR Recomm. Rep. 57, 1–20 (2008). Artz, A. S. et al. American Society of Clinical Oncology provisional clinical opinion: chronic hepatitis B virus infection screening in patients receiving cytotoxic chemotherapy for treatment of malignant diseases. J. Clin. Oncol. 28, 3199–3202 (2010). Lau, G. K. et al. Early is superior to deferred preemptive lamivudine therapy for hepatitis B patients undergoing chemotherapy. Gastroenterology 125, 1742–1749 (2003). Hsu, C. et al. A revisit of prophylactic lamivudine for chemotherapy‑associated hepatitis B reactivation in non‑Hodgkin’s lymphoma: 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. a randomized trial. Hepatology 47, 844–853 (2008). Loomba, R. et al. Systematic review: the effect of preventive lamivudine on hepatitis B reactivation during chemotherapy. Ann. Intern. Med. 148, 519–528 (2008). Ziakas, P . D., Karsaliakos, P Mylonakis, E. . Effect of prophylactic lamivudine for chemotherapy‑associated hepatitis B reactivation in lymphoma: a meta‑analysis of published clinical trials and a decision tree addressing prolonged prophylaxis and maintenance. Haematologica 94, 998–1005 (2009). Lok, A. S. McMahon, B. J. Chronic hepatitis B. Hepatology 45, 507–539 (2007). Hui, C. K. et al. Hepatitis B reactivation after withdrawal of pre‑emptive lamivudine in patients with haematological malignancy on completion of cytotoxic chemotherapy. Gut 54, 1597–1603 (2005). Yeo, W. Johnson, P Diagnosis, prevention . J. and management of hepatitis B virus reactivation during anticancer therapy. Hepatology 43, 209–220 (2006). Lau, G. K. et al. Preemptive use of lamivudine reduces hepatitis B exacerbation after allogeneic hematopoietic cell transplantation. Hepatology 36, 702–709 (2002). Lok, A. S. et al. Long‑term safety of lamivudine treatment in patients with chronic hepatitis B. Gastroenterology 125, 1714–1722 (2003). European Association For The Study Of The Liver. EASL Clinical Practice Guidelines: management of chronic hepatitis B. J. Hepatol. 50, 227–242 (2009). Evens, A. M. et al. Rituximab‑associated hepatitis B virus (HBV) reactivation in lymphoproliferative diseases: meta‑analysis and examination of FDA safety reports. Ann. Oncol. 22, 1170–1180 (2011). Onozawa, M. et al. Progressive disappearance of anti‑hepatitis B surface antigen antibody and reverse seroconversion after allogeneic hematopoietic stem cell transplantation in patients with previous hepatitis B virus infection. Transplantation 79, 616–619 (2005). Kawatani, T. et al. Incidence of hepatitis virus infection and severe liver dysfunction in patients receiving chemotherapy for hematologic malignancies. Eur. J. Haematol. 67, 45–50 (2001). Ozguroglu, M., Bilici, A., Turna, H. Serdengecti, S. Reactivation of hepatitis B virus infection with cytotoxic therapy in non‑Hodgkin’s lymphoma. Med. Oncol. 21, 67–72 (2004). Markovic, S., Drozina, G., Vovk, M. Fidler‑Jenko, M. Reactivation of hepatitis B but not hepatitis C in patients with malignant lymphoma and immunosuppressive therapy. A prospective study in 305 patients. Hepatogastroenterology 46, 2925–2930 (1999). Vento, S., Cainelli, F. Longhi, M. S. Reactivation of replication of hepatitis B and C viruses after immunosuppressive therapy: an unresolved issue. Lancet Oncol. 3, 333–340 (2002). Faggioli, P et al. Acute hepatic toxicity during . cyclic chemotherapy in non Hodgkin’s lymphoma. Haematologica 82, 38–42 (1997). Nosotti, L. et al. Hepatitis C virus infection prevalence and liver dysfunction in a cohort of B‑cell non‑Hodgkin’s lymphoma patients treated with immunochemotherapy. Scand. J. Infect. Dis. http://dx.doi.org/10.3109/ 00365548.2011.611819. Takai, S. et al. Prevalence of hepatitis B and C virus infection in haematological malignancies NATURE REVIEWS | CLINICAL ONCOLOGY 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. 59. 60. 61. and liver injury following chemotherapy. Eur. J. Haematol. 74, 158–165 (2005). de Pree, C., Giostra, E., Galetto, A., Perrin, L. Zulian, G. B. Hepatitis C virus acute exacerbation during chemotherapy and radiotherapy for oesophageal carcinoma. Ann. Oncol. 5, 861–862 (1994). Melisko, M. E., Fox, R. Venook, A. Reactivation of hepatitis C virus after chemotherapy for colon cancer. Clin. Oncol. (R. Coll. Radiol.) 16, 204–205 (2004). Fan, F. S. et al. Withdrawal of immunosuppressive therapy in allogeneic bone marrow transplantation reactivates chronic viral hepatitis C. Bone Marrow Transplant. 8, 417–420 (1991). Kanamori, H. et al. Case report: fulminant hepatitis C viral infection after allogeneic bone marrow transplantation. Am. J. Med. Sci. 303, 109–111 (1992). Zuckerman, E., Zuckerman, T., Douer, D., Qian, D. Levine, A. M. Liver dysfunction in patients infected with hepatitis C virus undergoing chemotherapy for hematologic malignancies. Cancer 83, 1224–1230 (1998). Mahale P et al. Acute exacerbation of chronic . hepatitis C in cancer patients. Presented at the 48th Annual Meeting of the Infectious Diseases Society of America (Vancouver, Canada, 2010). Vento, S. et al. Fulminant hepatitis on withdrawal of chemotherapy in carriers of hepatitis C virus. Lancet 347, 92–93 (1996). Nakamura, Y., Motokura, T., Fujita, A., Yamashita, T. Ogata, E. Severe hepatitis related to chemotherapy in hepatitis B virus carriers with hematologic malignancies. Survey in Japan, 1987–1991. Cancer 78, 2210–2215 (1996). Locasciulli, A. et al. Hepatitis reactivation and liver failure in haemopoietic stem cell transplants for hepatitis B virus (HBV)/hepatitis C virus (HCV) positive recipients: a retrospective study by the Italian group for blood and marrow transplantation. Bone Marrow Transplant. 31, 295–300 (2003). Hamaguchi, M. et al. Retrospective study on the impact of hepatitis B and hepatitis C virus infection on hematopoietic stem cell transplantation in Japan. Int. J. Hematol. 75, 324–331 (2002). Turner, N. C., Dusheiko, G. Jones, A. Hepatitis C and B‑cell lymphoma. Ann. Oncol. 14, 1341–1345 (2003). Nicot, F. et al. No evidence of occult hepatitis C virus (HCV) infection in serum of HCV antibody‑positive HCV RNA‑negative kidney‑transplant patients. Transpl. Int. 23, 594–601 (2010). McGovern, B. H. et al. Improving the diagnosis of acute hepatitis C virus infection with expanded viral load criteria. Clin. Infect. Dis. 49, 1051–1060 (2009). Arcaini, L. et al. Impact of treatment‑related liver toxicity on the outcome of HCV‑positive non‑Hodgkin’s lymphomas. Am. J. Hematol. 85, 46–50 (2010). Locasciulli, A. et al. Prevalence and natural history of hepatitis C infection in patients cured of childhood leukemia. Blood 90, 4628–4633 (1997). Gigliotti, A. R., Fioredda, F. Giacchino, R. Hepatitis B and C infection in children undergoing chemotherapy or bone marrow transplantation. J. Pediatr. Hematol. Oncol. 25, 184–192 (2003). Poynard, T., Yuen, M. F., Ratziu, V. Lai, C. L. Viral hepatitis C. Lancet 362, 2095–2100 (2003). VOLUME 9 | MARCH 2012 | 165 © 2012 Macmillan Publishers Limited. All rights reserved
- 11. REVIEWS 62. Pawlotsky, J. M. Use and interpretation of virological tests for hepatitis C. Hepatology 36 (Suppl. 1), 65–73 (2002). 63. Liang, R. How I treat and monitor viral hepatitis B infection in patients receiving intensive immunosuppressive therapies or undergoing hematopoietic stem cell transplantation. Blood 113, 3147–3153 (2009). 64. Francisci, D. et al. Management of hepatitis B virus reactivation in patients with hematological malignancies treated with chemotherapy. Infection 38, 58–61 (2010). 65. Peffault de Latour, R. et al. Allogeneic hematopoietic cell transplant in HCV-infected patients. J. Hepatol. 48, 1008–1017 (2008). 66. Keeffe, E. B. Hepatitis B virus reactivation with chemotherapy: diagnosis and prevention with antiviral prophylaxis. Rev. Gastroenterol. Disord. 4, 46–48 (2004). 67. Fong, T. L. et al. Short‑term prednisone therapy affects aminotransferase activity and hepatitis C virus RNA levels in chronic hepatitis C. Gastroenterology 107, 196–199 (1994). 68. Ciesek, S. et al. Glucocorticosteroids increase cell entry by hepatitis C virus. Gastroenterology 138, 1875–1884 (2010). 69. Magy, N. et al. Effects of corticosteroids on HCV infection. Int. J. Immunopharmacol. 21, 253–261 (1999). 70. Ennishi, D. et al. Monitoring serum hepatitis C virus (HCV) RNA in patients with HCV‑infected CD20‑positive B‑cell lymphoma undergoing rituximab combination chemotherapy. Am. J. Hematol. 83, 59–62 (2008). 71. Akiyama, H. et al. Effects of cyclosporin A on hepatitis C virus infection in bone marrow transplant patients. Bone Marrow Transplantation Team. Bone Marrow Transplant. 20, 993–995 (1997). 72. Anoop, P Wotherspoon, A. Matutes, E. ., Severe liver dysfunction from hepatitis C virus reactivation following alemtuzumab treatment for chronic lymphocytic leukaemia. Br. J. Haematol. 148, 484–486 (2010). 73. Gutierrez, M. L. et al. Cumulative dose of rituximab is a risk factor of HBV reactivation [abstract]. Hepatology 54 (Suppl. 1), a507 (2011). 74. Hsieh, C. Y. et al. Rituximab‑induced hepatitis C virus reactivation after spontaneous remission in diffuse large B‑cell lymphoma. J. Clin. Oncol. 26, 2584–2586 (2008). 75. Mahale, P Torres, H. A. Changes in hepatitis C . virus RNA levels in cancer patients undergoing chemotherapy or immunosuppressive therapy. Presented at the 49th Annual Meeting of the Infectious Diseases Society of America (Boston, Massachusetts, 2011). 76. Ennishi, D. et al. Does rituximab really induce hepatitis C virus reactivation? J. Clin. Oncol. 26, 4695–4696 (2008). 77. Foran, J. M. Hepatitis C in the rituximab era. Blood 116, 5081–5082 (2010). 166 | MARCH 2012 | VOLUME 9 78. Boyle, S. Reid, E. Viral reactivation and clinical hepatitis in patients with hepatitis C who receive rituximab as part of chemotherapy for treatment of lymphoma: A case series [abstract]. J. Clin. Oncol. 28 (Suppl.) e18559 (2010). 79. Sansonno, D. et al. Monoclonal antibody treatment of mixed cryoglobulinemia resistant to interferon alpha with an anti‑CD20. Blood 101, 3818–3826 (2003). 80. Torres, H., Mahale, P Ying, J. ., Kontoyiannis, D. P Rituximab and gemcitabine . are associated with acute exacerbation of chronic hepatitis C virus infection in patients with cancer [abstract]. Hepatology 54 (Suppl. 1), a1732 (2011). 81. Coppola, N. et al. Increased hepatitis C viral load and reactivation of liver disease in HCV RNA‑positive patients with onco‑haematological disease undergoing chemotherapy. Dig. Liver Dis. 44, 49–54 (2012). 82. Ferri, C., Govoni, M. Calabrese, L. The A, B, Cs of viral hepatitis in the biologic era. Curr. Opin. Rheumatol. 22, 443–450 (2010). 83. Cansu, D. U., Kalifoglu, T. Korkmaz, C. Short‑term course of chronic hepatitis B and C under treatment with etanercept associated with different disease modifying antirheumatic drugs without antiviral prophylaxis. J. Rheumatol. 35, 421–424 (2008). 84. Mahale P Kaseb A., Davila M. Torres H. A. The ., effect of transcatheter arterial chemoembolization on hepatitis C virus kinetics in patients with HCV associated hepatocellular carcinoma [abstract]. J. Clin. Oncol. 29 (Suppl.), e14578 (2011). 85. Maruta, A. et al. Liver function tests of recipients with hepatitis C virus infection after bone marrow transplantation. Bone Marrow Transplant. 13, 417–422 (1994). 86. Ljungman, P et al. Long‑term effects of . hepatitis C virus infection in allogeneic bone marrow transplant recipients. Blood 86, 1614–1618 (1995). 87. Kawatani, T., Tajima, F., Ishiga, K., Suou, T. Kawasaki, H. Liver dysfunction in patients with acute myelogenous leukemia: studies on patients not infected with hepatitis C virus during intense therapy. J. Med. 29, 45–56 (1998). 88. Kawatani, T., Suou, T., Tajima, F., Ooi, S. Kawasaki, H. Hepatitis C virus infection in acute leukemia with liver dysfunction. Eur. J. Haematol. 51, 254–255 (1993). 89. Besson, C. et al. Characteristics and outcome of diffuse large B‑cell lymphoma in hepatitis C virus‑positive patients in LNH 93 and LNH 98 Groupe d’Etude des Lymphomes de l’Adulte programs. J. Clin. Oncol. 24, 953–960 (2006). 90. Gruber, A., Lundberg, L. G. Bjorkholm, M. Reactivation of chronic hepatitis C after withdrawal of immunosuppressive therapy. J. Intern. Med. 234, 223–225 (1993). 91. Firpi, R. J. Nelson, D. R. Management of viral hepatitis in hematologic malignancies. Blood Rev. 22, 117–126 (2008). 92. Visco, C. et al. Distinctive natural history in hepatitis C virus positive diffuse large B‑cell lymphoma: analysis of 156 patients from northern Italy. Ann. Oncol. 17, 1434–1440 (2006). 93. Torres, H. A. et al. Hepatitis C virus infection in cancer patients: the story of a forgotten population. Presented at the 48th Annual Meeting of the Infectious Diseases Society of America (Vancouver, Canada, 2010). 94. Huang, J. F. et al. The efficacy and safety of pegylated interferon plus ribavirin combination therapy in chronic hepatitis C patients with hepatocellular carcinoma post curative therapies—a multicenter prospective trial. J. Hepatol. 54, 219–226 (2011). 95. Ghany, M. G., Nelson, D. R., Strader, D. B., Thomas, D. L. Seeff, L. B. An update on treatment of genotype 1 chronic hepatitis C virus infection: 2011 practice guideline by the American Association for the Study of Liver Diseases. Hepatology 54, 1433–1444 (2011). 96. Torres, H. A. et al. Hepatitis C clinic operated by infectious disease at a comprehensive cancer center—help is on the way. Clin. Infect. Dis. (in press). 97. Papaevangelou, V. et al. Hepatitis C treatment concomitant to chemotherapy as “salvage” therapy in children with hematologic malignancies. Pediatr. Infect. Dis. J. 29, 277–280 (2010). 98. Tomblyn, M. et al. Guidelines for preventing infectious complications among hematopoietic cell transplantation recipients: a global perspective. Biol. Blood Marrow Transplant. 15, 1143–1238 (2009). 99. Ghany, M. G., Strader, D. B., Thomas, D. L. Seeff, L. B. Diagnosis, management, and treatment of hepatitis C: an update. Hepatology 49, 1335–1374 (2009). 100. Moradpour, D., Penin, F. Rice, C. M. Replication of hepatitis C virus. Nat. Rev. Microbiol. 5, 453–463 (2007). 101. Gravitz L. Introduction: a smouldering publichealth crisis. Nature 474, S2–S4 (2011). Acknowledgments We thank Stephanie P Deming, scientific editor at the . Department of Scientific Publications at the MD Anderson Cancer Center, for editorial assistance. No funding sources were involved in the writing of this Review or the decision to submit the Review for publication. Author contributions Both authors researched data for the article, made substantial contributions to the discussion of content, wrote the article, and reviewed and edited the manuscript before submission. www.nature.com/nrclinonc © 2012 Macmillan Publishers Limited. All rights reserved