Implant Over dentures by Dr. Ajay Vikram Singh
•
2 gostaram•1,716 visualizações

Here is my article on implant over denture published in Dental Practice journal, south east Asia edition. I believe this article will help both the dentists and well as the needy patients to understand the quality life after the implant supported over dentures. For more information and to consult for the similar or any implant procedure pls write me at my id drajaydentalclinic@gmail.com you can also visit my websites to know more about our implant treatment options and implant training programs. our websites are www.dentalimplantclinicindia.com and www.implanttrainingindia.com

Recomendados
Recomendados
Mais conteúdo relacionado
Último
Último (20)
Destaque
Destaque (20)
Implant Over dentures by Dr. Ajay Vikram Singh
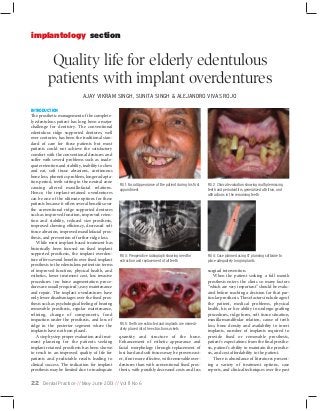
- 1. implantology section Quality life for elderly edentulous patients with implant overdentures AJAY VIKRAM SINGH, SUNITA SINGH & ALEJANDRO VIVAS ROJO INTRODUCTION The prosthetic management of the completely edentulous patient has long been a major challenge for dentistry. The conventional edentulous ridge supported dentures, well over centuries, has been the traditional standard of care for these patients but most patients could not achieve the satisfactory comfort with the conventional dentures and suffer with several problems such as inadequate retention and stability, inability to chew and eat, soft tissue abrasions, continuous bone loss, phonetics problem, longer adaptation period, teeth setting in the neutral zone causing altered maxillofacial relations. Hence, the implant-retained overdentures can be one of the ultimate options for these patients because it offers several benefits over the conventional ridge supported dentures such as improved function, improved retention and stability, reduced size prosthesis, improved chewing efficiency, decreased soft tissue abrasion, improved maxillofacial prosthesis, and prevention of further ridge loss. While most implant-based treatment has historically been focused on fixed implant supported prosthesis, the implant overdenture offers several benefits over fixed implant prosthesis to the edentulous patients in terms of improved function, physical health, and esthetics, lower treatment cost, less invasive procedures (no bone augmentation procedures are usually required), easy maintenance and repair. The implant overdentures have only fewer disadvantages over the fixed prosthesis such as psychological feeling of bearing removable prosthesis, regular maintenance, relining, change of components, food impaction under the prosthesis, and loss of ridge in the posterior segment where the implants have not been placed. A step by step proper evaluation and treatment planning for the patients seeking implant retained prosthesis has been shown to result in an improved quality of life for patients and predictable results leading to clinical success. The indication for implant prosthesis may be limited due to inadequate FIG 1: Facial Appearance of the patient during his first appointment FIG 2: Clinical evaluation showing multiple missing teeth and periodontitis, generalized attrition, and abfractions in the remaining teeth FIG 3: Preoperative radiograph showing need for extraction and replacement of all teeth FIG 4: Case planned using CT planning software to place adequately long implants FIG 5: Teeth are extracted and implants are immediately placed into the extraction sockets quantity and structure of the bone. Enhancement of esthetic appearance and facial morphology through replacement of lost hard and soft tissues may be proven easier, if not more effective, with removable overdentures than with conventional fixed prosthesis, with possibly decreased costs and less 22 Dental Practice // May-June 2013 // Vol 11 No 6 surgical intervention. When the patient seeking a full mouth prosthesis enters the clinic so many factors “which are very important” should be evaluated before reaching a decision for that particular prosthesis. These factors include age of the patient, medical problems, physical health, his or her ability to undergo grafting procedures, ridge form, soft tissue situation, maxilla-mandibular relation, cause of teeth loss, bone density and availability to insert implants, number of implants required to provide fixed or removable prosthesis, patient’s expectations from the final prosthesis, patient’s ability to maintain the prosthesis, and cost affordability to the patient. There is abundance of literatures presenting a variety of treatment options, case reports, and clinical techniques over the past
- 2. FIG 6 & 7: Peri-implant socket spaces are grafted, transgingival healing abutments are immediately placed on top of implants and sutures are placed to approximate the soft tissue FIG 8: Healing after 6 weeks FIG 9: Denture FIG 10: Posterior teeth are extracted one week before the denture placement 30 years, but there is a general consensus about the treatment protocols and long term documented benefits of implant overdentures. In the author’s clinical practice, this treatment option has become the most rewarding care for the edentulous elderly patients with increased life expectancy and chewing benefits. Although there still remains a lack of consistency in terms of techniques, prosthetic design, and attachment systems, these aspects have been proven less important to successful outcomes than once thought. there was almost complete loss of vertical bone dimension in the posterior maxilla due to long time edentulism in the region and sinus pneumatization. In the mandibular posterior segments the teeth were intact but showed large osseo-defects which mandate the grafting procedures to place adequately sized implants in the region (Figure 3). In the anterior maxilla, the teeth number 21, 22, and 23 showed exposed canals with tooth number 21 showing periapical radiolucency in the radiograph but teeth were asymptomatic clinically. After clinical and radiographic evaluations, the authors reached the decision for the extraction of all remaining teeth and placement of full mouth prosthesis. Now to present various replacement options, the patient was evaluated for his physical health, medical problems, and financial status to bear the treatment cost. On general evaluation and medical history, it was found that the patient was fit for the dental implant procedure. To confirm medical fitness, blood investigations were done for general blood picture, blood sugar level (random), thyroxin along with blood pressure and ECG. Various options were now offered to the patient for teeth replacement. Keeping in mind various aspects such as his age, poor oral hygiene maintenance habit, heavy bite CASE REPORT Examination and Treatment Planning A 70 year old male patient reported at our clinic for the replacement of a few missing teeth and treatment of his periodontically diseased teeth (Figure 1). On clinical evaluation, it was found that the patient had lost a couple of his teeth because of periodontitis and remaining teeth showed signs of periodontal disease such as periodontal pockets and mobility. It was also found that the patient has generalized attrition and abfractions due to heavy bite forces on the teeth (Figure 2). On radiographic evaluation (panoramic radiograph), the periodontal bone loss was found with most of the remaining teeth. An abundant bone height was seen in the anterior segment of both arches but forces and inadequate bone in posterior segments to insert implants, affordability and patient’s expectations from the new prosthesis, the implant retained over denture was finalized as the definitive treatment option. To evaluate the exact bone dimensions and bone density, the CT planning was done for the patient using Implant 3D software so that adequately long and wide implants can be inserted with minimal surgical intervention and stabilized into the cortex to achieve adequate initial stability (Figure 4). Based on CT planning, placement of three long implants (3.75 x 18) in the anterior mandible and four implants (3.75 x 18) in the anterior maxilla immediately into the extraction sockets were planned. After the dental hygiene appointments for scaling and root planing to eradicate the deep pockets and minimize infection to the implants, the case was scheduled for the implant surgery. The patient was prescribed tab Valium 5mg at night before the surgery for sound sleep and tab Augmentin (1 gm) one hour before the implant surgery. CLINICAL PROCEDURES The anterior teeth were extracted with minimal trauma to the alveolar bone and soft tissue and the granulation tissue was curetted out from the sockets. The extraction sockets were irrigated with parental form of clindamycin to kill all the residual pathogens in the sockets before implant osteotomy preparations. The implant osteotomies were prepared through the sockets to reach the basal bones (nasal floor and base of the mandible). All the implants were stabilized into the cortex to achieve high initial stability (more than 40 Ncm), hence the transmucosal abutments were immediately screwed on top of implants (transgingival implant placement/ single stage implant surgery). The periimplant socket spaces were grafted using synthetic bone Dental Practice // May-June 2013 // Vol 11 No 6 23
- 3. implantology section FIG 11 & 12: Healing abutments are removed and replaced with ball attachments FIG 13 & 14: Plastic caps are seated into the metal cap plastic ball caps; female part are seated into the metal ball caps (Figures 13 & 14). The ball caps are seated on top of ball attachments in the mouth (Figure 15). The tissue surface of the denture is hollowed at the site of implants to accommodate the ball caps (Figure 16). The dentures are tried in the mouth for their complete seating over the ball caps (Figure 17). A piece of rubber dam sheath is placed under the metal balls to avoid the self cure resin to get flow and locked into the undercuts (Figure 18). The self cure acrylic resin is mixed and filled into the tissue surface of the dentures and dentures are seated in the mouth in the correct occlusion (Figure 19). Authors would like to mention here that the separating media (petroleum jelly) was applied over the denture except the tissue surface to avoid sticking of the acrylic over the teeth and flanges. Once the acrylic hardens, the dentures were removed from the mouth. The ball caps came out embedded within the tissue surface of the dentures (Figure 20). The palatal extension of maxillary denture is removed and flanges are short- FIG 15: Caps are placed onto the ball attachments in patient’s mouth FIG 16 & 17: Tissue surface of the denture is hollowed to make space of the ball caps substitute (HA+ β-Tcp). No barrier membrane was used. The sutures were placed to approximate the tissue to fasten healing and to prevent loss of graft (Figure s5-7). Posterior teeth were extracted but a couple of teeth which were in occlusion were left to maintain the same chewing efficiency and also to record the same jaw relations for denture fabrication. Patient was put on antibiotics and analgesics only for 3 days postoperatively. An interim removable prosthesis was given to the patient for his anterior segments which got stabilized onto the healing abutments. Patient was recalled after 6 weeks for the denture fabrication, when soft tissue was healed and implant achieved secondary sta- bility into the bone (Figure 8). Impressions were made and bite registration was done. Maxillary and mandibular models were articulated using semi adjustable articulators, teeth removed from the models and teeth setting was done. The final denture was fabricated in the laboratory (Figure 9). Patient was recalled and the remaining teeth were extracted. When the extraction sockets got primarily healed in a weeks time, patient was recalled for the final denture delivery (Figure 10). The transmucosal healing abutments are removed from the implants and replaced with the appropriate sized ball abutments; male part (Figures 11 & 12). The ball attachments are finally tightened to 35Ncm using torque ratchet to avoid future loosening. The 24 Dental Practice // May-June 2013 // Vol 11 No 6 ened (Figure 21). The dentures are finished and polished and seated over the implants in the mouth (Figure 22 & 23). A post-loading panoramic radiograph was done to evaluate the accurate seating of the denture components (Figure 24). The patient experienced an outstanding satisfaction in denture retention, stability, chewing efficacy, improved maxillofacial relations (improved appearance) from day one after placing the implant retained dentures in mouth (Figure 25). CONCLUSION Conventional ridge supported dentures have been used as the only standard of care for decades but implant supported overdenture offers numerous benefits over the
- 4. FIG 18: Piece of rubber dam is placed to block the undercuts under the ball caps FIG 19: Self cure resin is filled into the denture and dentures are seated in mouth in occlusion over the ball caps FIG 21: Palatal extension and denture flanges are removed FIG 22 & 23: Finally finished and polished dentures seated in the patient’s mouth patient evaluation, treatment planning, ideal communication among surgical, laboratory, and restorative colleagues, implant overdentures provide simple, predictable, and cost-effective treatment to edentulous patients. Additionally, they provide the FIG 20: Dentures are removed from the mouth after the acrylic has set carrying the ball caps embedded within the dentures benefits of esthetics, phonetics, bone preservation, increased comfort, better psychosocial state, and enhanced nutrition, all resulting in an improved quality of life. For a complete list of references, email info@dental-practice.biz About the AUTHORS FIG 24: Post loading radiograph FIG 25: A satisfied patient with great satisfaction after using implant over dentures conventional dentures in terms of improved retention, improved chewing efficacy, improved maxillofacial relations, improved speech, reduced size prosthesis and much more. Through meticulous Dr. Ajay Vikram Singh after his graduation in dentistry and receiving PG. certificate training in Implantology from India, received advanced level implant training at various centers and continuing education programmes in USA. He also received continuing education in implantology at the School of Dentistry, The University of Queensland in Australia. Currently, He is an internationally acclaimed mentor, speaker and researcher in the field of implantology. He has spoken as the key note speaker in the various national and international implant conferences in India and abroad. Besides being the active member of various prestigious implant associations, he is the fellow and Diplomate of international congress of implantology (ICOI). He is the founder president of International Academy of Implant Dentistry. Dr. Ajay has authored a dental implant book Title “Clinical Implantology” Published worldwide with “Elsevier”. Dr. Ajay is the founder of International Implant Training Centre (IITC), Agra where he trains several dentists from India and abroad in basic and advanced level implantology. Dr. Ajay does the private practice at Dr. Ajay Dental Clinic & Research Centre, Agra. He can be reached at drajaydentalclinic@gmail.com Dr. Sunita Singh received continuing education in esthetic and implant dentistry, and fixed orthodontics at various centers in India and USA. She has attended and presented in many national and international dental conferences. She has received training in Cosmetic Dentistry from Washington University (USA). She is a member of American College of Prosthodontists in USA. She is a member of various prestigious implant associations and has co-authored the text book in implantology title “Clinical Implantology”. She has been practicing with Dr. Ajay Vikram Singh since 2003 at Dr. Ajay Dental Clinic and Research Center, Agra. Alejandro Vivas Rojo. DDS Ms. (Venezuela) is an Oral and Maxillofacial Surgeon. Member, American Association of Oral and Maxillofacial Surgery. He is attending Surgeon at Hospital dos Lusiadas; Oral and Maxillofacial Service. Lisbon-Portugal. Dental Practice // May-June 2013 // Vol 11 No 6 25