Pancreas Cancer
•Transferir como PPTX, PDF•
212 gostaram•102,562 visualizações

Understanding pancreas cancer, including the causes, symptoms, diagnostic tests and the best treatment options for this very serious malignancy

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Pancreas Cancer
Semelhante a Pancreas Cancer (20)
Mais de Robert J Miller MD
Mais de Robert J Miller MD (20)
Último
Último (20)
Pancreas Cancer
- 2. Pancreas Cancer Incidence (2014 Data) Deaths 46,420 (2.8%) 39,590 (6.8%) The 5 year survival is only 6.7% Life time risk of developing this cancer is 1.5%
- 3. 2014 Statistics Male Female New Cases 23,530 (2.7%) 22,890 (2.8%) Deaths 20,170 (6.5%) 19,420 (7%)
- 4. Age and Pancreas Cancer Median age is 71
- 5. New Cases per 100,000
- 6. Trends in Incidence and Survival
- 7. Stage and Survival - SEER Stage Incidence Survival/5y Local 9% 25.8% Regional 28% 9.9% Distant 53% 2.3%
- 8. Risk factors for pancreatic cancer include the following - Smoking - Obesity - Personal history of diabetes or chronic pancreatitis - Family history of pancreatic cancer or pancreatitis - Certain hereditary conditions
- 9. Symptoms Most patients present with pain (in the back) weight loss or jaundice Tumors in the head of the pancreas are more likely to have jaundice, Those that arose in the body or tail, more likely pain and weight loss.
- 10. Bile: yellowish fluid produced in the liver that aids in digestion of fat in the small intestine Liver
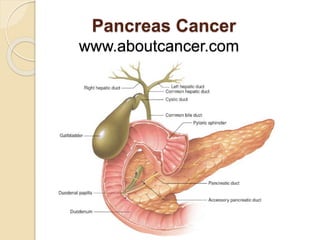
- 11. Bile: passes through the common bile duct through the head of the pancreas on it’s way to the duodenum Liver Hepatic Duct Common Bile Duct Duodenum Pancreatic Duct
- 12. Bile duct carries the bilirubin through the head of the pancreas on it’s way to the duodenum Tail of the Pancreas Common Bile Duct Common Bile Duct Body of the Pancreas Head of the Pancreas
- 13. Tumors in the head of the pancreas are more likely to have jaundice Tail of the Pancreas Common Bile Duct Common Bile Duct Body of the Pancreas Head of the Pancreas Tumor in the Head of the Pancreas Obstruct the Bile Duct
- 14. Tumors in the head of the pancreas are more likely to have jaundice Tail of the Pancreas Common Bile Duct Common Bile Duct Body of the Pancreas Head of the Pancreas Pancreatic Duct Tumor in the Head of the Pancreas
- 15. Head of the Pancreas Tumor Blocking the pancreatic duct and common bile duct Common bile Duct Pancreatic duct Common bile Duct cancer Duodenum
- 16. Tail of the Pancreas Common Bile Duct Common Bile Duct Body of the Pancreas Head of the Pancreas Tumor Tumors in the body or tail are more likely to present with pain or weight loss
- 17. Symptoms of Pancreas Cancer • Asthenia (weakness) – 86 percent • Weight loss – 85 percent • Anorexia (no appetite)– 83 percent • Abdominal pain – 79 percent • Epigastric pain (stomach) – 71 percent • Dark urine – 59 percent • Jaundice – 56 percent • Nausea – 51 percent • Back pain – 49 percent • Diarrhea- 44 percent • Vomiting – 33 percent • Steatorrhea (fatty stools)– 25 percent • Thrombophlebitis – 3 percent
- 18. Signs of Pancreas Cancer • Jaundice (yellow) – 55 percent • Hepatomegaly (large liver) - 39 percent • Right upper quadrant mass – 15 percent • Cachexia (wasting) – 13 percent • Courvoisier’s sign (nontender but palpable distended gallbladder at the right costal margin) – 13 percent • Epigastric mass (fell lump in stomach) – 9 percent • Ascites (abdominal fluid) – 5 percent
- 19. Pathology Ductal adenocarcinoma accounts for about 85% of all neoplasms. And more than 95% of all pancreatic cancers arise from the exocrine (digestive enzymes) elements. Cancers that arise from the endocrine cells (neuroendocrine, islet cells) account for 5% or less
- 20. Parts of the Pancreas Portal Vein Aorta Superior Mesenteric Vein Head Body Tail
- 21. Cancer in the Head of the Pancreas Head Tail Body
- 22. Location of Pancreas Cancer • 60 to 70 percent of exocrine pancreatic cancers are localized to the head • 20 to 25 percent are in the body/tail and • the remainder involve the whole organ H = Head N = Neck B = Body T = Tail Un = Uncinate
- 23. Location of Pancreas Cancer • 60 to 70 percent of exocrine pancreatic cancers are localized to the head • 20 to 25 percent are in the body/tail and • the remainder involve the whole organ H = Head N = Neck B = Body T = Tail Un = Uncinate
- 24. Tests used to evaluate and stage pancreas cancer • Routine blood tests e.g. liver products like bilirubin • Elevated tumor markers (CA 19-9 or CEA) • MRI, CT scans, Ultrasound • Endoscopy including endoscopic ultrasound or ERCP • Laparoscopy • Biopsy
- 25. CA 19-9 The reported sensitivity and specificity rates of CA 19-9 for pancreatic cancer range from 70 to 92, and 68 to 92 percent, respectively. The rates of unresectable disease among all patients with a CA 19-9 level ≥130 units/mL versus <130 units/mL were 26 and 11 percent, respectively. Among patients with tumors in the body/tail of the pancreas, more than one-third of those who had a CA 19-9 level ≥130 units/mL had unresectable disease.
- 26. Elevated CA 19-9 Cancer - Pancreas - Biliary Cancer (gallbladder, cholangiocarcinoma, ampullary) - Hepatocellular - Gastric, ovarian, colorectal (less often) - Lung, breast, uterus (rare) Benign - Acute cholangitis - Cirrhosis and other cholestatic diseases (gall stones)
- 27. Ultrasound study of 900 patients who underwent ultrasound to work up painless jaundice, anorexia, or unexplained weight loss The sensitivity for detection of all tumors in the pancreas was 89 percent Among the 779 patients who were followed over time and established not to have developed a pancreatic tumor, nine had false-positive US findings (specificity 99 percent).
- 28. Ultrasound Mass in the pancreatic head and dilated common bile duct and pancreatic duct
- 29. CT Sensitivity of CT for pancreatic cancer depends on technique and is highest (89 to 97 percent) with triple-phase, helical multidetector row CT As expected, sensitivity is higher for larger tumors; in one study, the sensitivity was 100 percent for tumors >2 cm, but only 77 percent for tumors ≤2 cm in size
- 30. Endoscopy or ERCP or EUS
- 31. ERCP or Endoscopic retrograde cholangiopancreatography Scope Duodenum
- 32. ERCP Try to get into the duct system
- 33. ERCP Inject dye into the duct system and look for compression
- 34. ERCP Sensitivity of 92 percent and Specificity of 96 percent for diagnosing cancer of the pancreas by ERCP ERCP provides an opportunity to collect tissue samples (forceps biopsy, brush cytology) for histologic diagnosis. However, the sensitivity for detection of malignancy (approximately 50 to 60 percent) is lower than that of endoscopic ultrasound (EUS)-guided FNA (sensitivity 92 percent)
- 35. endoscope EUS (Endoscopic Ultrasound Ultrasound Tip Detailed image of this area
- 36. EUS or Endoscopic Ultrasound A: met to the pancreas head B: lymphoma in tail C: endocrine tumor in isthmus D: insulinoma in body From Endoscopic Ultrasound 2014:3
- 37. EUS used for pain relief with celiac plexus neurolysis
- 38. Endoscopic Placement of a Stent cancer stent duct pancreas stent scope
- 39. CT Scan – Pancreas Cancer
- 40. CT Scans
- 41. CT or PET Scan
- 43. PET Scans
- 44. TNM Stage: how far has the cancer spread, T (tumor) N (nodes) M (mets) combine all 3 to get Stage
- 46. Stage IB (T2N0M0) over 2cm, limited to pancreas
- 47. Stage IIA (T3N0) beyond the pancreas
- 49. Stage III (T4) Unresectable Cancer has spread to the major blood vessels near the pancreas. These include the superior mesenteric artery, celiac axis, common hepatic artery, and portal vein.
- 51. Stage IV - Metastasis Lung Liver Peritoneal Cavity Cancer in Pancreas
- 52. NCDB Statistics Stage Incidence Survival/5y I 8.5% 20% II 23% 10% III 14% 2.5% IV 54% 1.6%
- 53. 1.2 1 0.8 0.6 0.4 0.2 0 Survival by Stage 0 year 1 year 2 year 3 year 4 year 5 year Stage I Stage II Stage III Stage IV
- 54. Survival Surgery offers the only cure but only 10-20% are candidates for resection and even in this group the 5 year survival is only 20% and the median 13 to 20 months Locally advanced the survival is 8 to 14 months Up to 60% already have metastases and a median survival of only 4 to 6 months
- 56. nccn.org
- 58. Summary of Treatment 1.Resection is the only chance for a cure, and resectable patients show undergo surgery without delay followed by adjuvant therapy 2.Borderline resectable patients may benefit from neoadjuvant therapy and then surgery 3.Unresectable patients may benefit from chemotherapy or chemoradiation 4.Metastatic disease may benefit from chemotherapy or other palliative treatments
- 59. Allen Oldfather Whipple (1881- 1963) Surgery professor at Columbia where he developed the resection for pancreas cancer in 1935 now called the Whipple Procedure
- 60. Summary of Treatment 1.Resection is the only chance for a cure, and resectable patients show undergo surgery without delay followed by adjuvant therapy 2.Borderline resectable patients may benefit from neoadjuvant therapy and then surgery 3.Unresectable patients may benefit from chemotherapy or chemoradiation 4.Metastatic disease may benefit from chemotherapy or other palliative treatments
- 61. Chemotherapy
- 62. Chemotherapy for Metastatic Pancreas Cancer • FOLFIRINOX (oxaliplatin (Eloxatin), irinotecan (Camptosar) , leucovorin, fluorouracil) • Gemzar (gemcitabine) + Abraxane (albumin bound paclitaxel) • Gemzar + erlotanib (Tarceva, EGFR drug)
- 63. Chemotherapy Survival Comparisons in Months 5-FU 4.4 Gemzar 5.6 Gemzar 6.8 FOLFIRINOX 11.1 Gemzar 6.7 Gem + Abraxane 8.7
- 64. Survival with Metastatic Pancreas Cancer FOLFIRINOX Months Gemzar NEJM 2011:364:1817
- 65. Survival with Metastatic Pancreas Cancer Gemzar + Abraxane Months Gemzar NEJM 2013;369:1691