Presentation1.pptx. radiological imaging of epilepsy.
•Transferir como PPTX, PDF•
44 gostaram•5,794 visualizações


Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Presentation1.pptx. radiological imaging of epilepsy.
Semelhante a Presentation1.pptx. radiological imaging of epilepsy. (20)
Mais de Abdellah Nazeer
Mais de Abdellah Nazeer (20)
Último
Último (20)
Presentation1.pptx. radiological imaging of epilepsy.
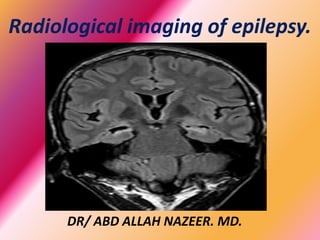
- 1. Radiological imaging of epilepsy. DR/ ABD ALLAH NAZEER. MD.
- 2. Epilepsyis a chronic neurological disorder characterized by spontaneous and recurrent seizures due to excessive and abnormal electrical activity of cortical neurons. It affects about 1% of population. Epilepsy diagnosis is purely clinical but neuroimaging, especially structural magnetic resonance (MR), plays a key role to rule out (and characterize) anatomic abnormalities and for treatment planning. Seizures are divided into generalized and partial. Generalized seizures usually originate in both cerebral hemispheres and most of them have a good response to antiepileptic drugs. Partial seizures (focal) most likely originate in one anatomical region and are classified as simple (when there is no loss of consciousness) and complex (when loss of consciousness is associated).
- 10. The role of CT in the assessment of epilepsy has considerably diminished and is viewed as supplementary or supportive. CT can be used as an initial screening method for excluding a brain neoplasm as a cause for seizure activity, but usually MRI is more appropriate in addition to avoiding irradiation. CT is ideal for identifying the presence and extent of intracranial calcification, but this has a limited impact on patient management. CT is not as sensitive as MRI at identifying small lesions and more subtle structural changes such as those involving the temporal lobe and focal cerebral dysplasia. There is also a role in the acute phase of status epilepticus, when cerebral edema secondary to hypoxia or anoxia is suspected. C.T
- 11. Hippocampal sclerosis (mesial temporal sclerosis). Mesial temporal sclerosis is the most common epileptogenic abnormality found after surgery in several series of epilepsy (65%) and the most important cause of refractory epilepsy. The most important MRI findings in hippocampal sclerosis are atrophy and increased signal intensity in long TR sequences . There are also other findings that we should look for because, although they are less important, they can help us to support the diagnosis. These findings are: the loss of the internal hippocampus architecture (which is best viewed with 3T machines), fornix and ipsilateral mammillary body atrophy (usually long-standing cases), ipsilateral temporal horn dilation, decreased of para-hippocampal white matter and reduced temporal lobe volume. In 8-20% cases of hippocampal sclerosis, dual pathology will be found, i.e. hippocampal sclerosis associated to other epileptogenic lesion, which is usually located outside the hippocampus.
- 12. Lesions most commonly associated are cortical development abnormalities, but tumours, post- traumatic gliosis or infectious residual lesions can be found. In up to 65% of cases of hippocampal sclerosis, white matter of the temporal pole has a subtle signal alteration (hyperintensity signal on FLAIR images) sometimes with gray-white matter junction blurred. It is important to identify these structural alterations that may be associated with hippocampal sclerosis because lesionectomy and hipocampectomía (when possible) have a greater benefit in seizure control.
- 13. Hippocampal sclerosis are atrophy and increased signal intensity.
- 17. Right hippocampal sclerosis with right temporal cortical dysplasia.
- 18. Malformations of cortical development (MCD) Second cause of anatomic abnormality found in surgical series of patients with chronic epilepsy. MCD are particularly common when the beginning of the crisis occurs in childhood. They occur as a result of defects in the different phases of cortical development: 1. Proliferation / Apoptosis of neuroblasts from the germinal matrix. 2. Migration (radial, tangential). 3. Organization of the cortex in sheets with neural network and synapses formation. About 15% of patients with MCD have seizures refractory to medical treatment and surgery may be the definitive treatment. In the case of diffuse alterations, surgical treatment is ineffective, contrary to focal lesions. In general, the degree of damage is related to the extension of the malformation. Barcovich classification of MCD provides four groups depending on the stage of development predominantly affected:
- 20. Malformations of cortical development (MCD)
- 21. GROUP I (malformations due to abnormal proliferation or apoptosis). - MICROCEPHALY. It may be primary (genetic) or secondary. - HEMIMEGALOENCEPHALY (HE). FOCAL CORTICAL DYSPLASIA (FCD) TYPE II. It associated with subtle focal changes which sometimes apparent microscopically. Seizures with type 11 FCD is high. Type1 FCD may or not present with epilepsy. - TUBEROUS SCLEROSIS. AD inherited disorder with classic clinical triad: facial angiofibromas, mental retardation and refractory seizures. Underlying pathogenetic: cortical tubers, subependymal nodules and subependymal giant cell astrocytomas. - TUMORS. Ganglioglioma. Desmoplastic infantile ganglioglioma. Gangliocytoma. Disembrioplastic neuroepithelial tumour.
- 22. Extreme Microcephaly, Diffuse Agyria, Agenesis of Corpus Callosum, Cerebellar Hypoplasia with Dandy-Walker Malformation:
- 23. Hemimegalencephaly with enlarged, dysmorphic LT. hemisphere, enlarged l left lateral ventricle with heterotopia and abnormal white matter.
- 26. Ganglioglioma.
- 27. Gangliocytoma Associated with Focal Cortical Dysplasia
- 28. GROUP II (malformations due to abnormal neuronal migration). - LISSENCEPHALY. MCD caused by the arrest of neuronal migration developing cerebral cortical thickening and smooth surface. Important overlap with band heterotopy. In image, particularly MRI, the cerebral hemispheres appear as "eight" or "hourglass" Number of cortical sulci separated by broad gyres, enlarged ventricles, truncated arborisation of the white matter. In infants, on T2 weighted-images can distinguish three layers:
- 30. LISSENCEPHALY.
- 31. HETEROTOPYS (HT). Alteration / arrest migration of groups of neurons from the periventricular germinal zone to the cortex, appearing as gray substance anywhere outside the cortex, from the ventricles to the meningeal coating, with size, morphology and location variable: 1. Periventricular / subependymal nodular HT (the most common). Uni or multifocal asymmetric indentation. 2. Band HT ("double cortex"). Symmetric thick band of subcortical gray matter. 3. Subcortical nodular HT. • Isolated nodules. Thin surface cortex often. • "Mass" of white matter that continues the cortex and the ventricular surface. 4. Periventricular and subcortical HT associated. CT and MRI show heterotopys similar to the cortex in density and signal intensity respectively . The ipsilateral hemisphere is small and the lateral ventricle is usually large due to underdevelopment of white matter.
- 32. GROUP III (malformations due to abnormal cortical organization) - POLYMICROGYRIA. MDC due to an anomaly in the late stages of neuronal migration and cortical organization. Convolutions formed are numerous, small, prominent and irregular. T2-weighted MRI has two patterns: • <12 months: cortex with fine and small ripples, normal thickness. •> 18 months: thick and irregular cortex, increase of Virchow-Robin spaces and variable cortical invagination.
- 33. HETEROTOPIA
- 38. Polymicrogyria:
- 41. - SCHIZENCEPHALY (E). Alteration in cortical organization characterized by the presence of clefts in the cerebral parenchyma, which extend from the cortical surface to the ventricular system coating with dysplastic gray matter. Often associated with polymicrogyria, heterotopy and microcephaly. There are two types: • E. "Closed lip": walls oppose one another, obliterating the subarachnoid space. Irregular gray matter cord extending from the cortical surface to the ventricle. • E. "Open-lip": CSF fills the cleft from the lateral ventricle to the subarachnoid space. At MRI gray matter coating can be more difficult to distinguish from that in the "closed Lip” The most common location is close to the pre and post-central gyrus. More often is unilateral than bilateral. Venous developmental anomalies are common in the cleft.
- 42. SCHIZENCEPHALY.
- 44. FOCAL CORTICAL DYSPLASIA (FCD) TYPE I. It is characterized by greater extension than the type II, affects more than one lobe and associates loss of white matter volume, without thickening or distortion the cortical pattern. Juxtacortical white matter shows discrete increase signal intensity especially in FLAIR and effacement of the SG / SB union differentiation. These findings are more difficult to detect than in type II FCD. It is most commonly located in the temporal lobe and may be associated with mesial sclerosis (dual pathology). The surgical outcome is worse due to its greatest extent and worse definition.
- 45. FCD Palmini type in the frontal lobe.
- 48. FCD at right parietal region.
- 49. Transmantle dysplasia compromising the right frontal cortex.
- 50. Neoplasms. The neoplasms may also cause drug-resistant epilepsy. About 90% of neoplasms that produce seizures will be located next to the cerebral cortex and of these, 70% are located in the temporal lobes. They tend to be low- grade neoplasm and slow growth usually without edema or mass effect associated. They can produce thinning or remodeling adjacent calvarium. Enhancement after intravenous contrast is common but may not be present. Oligodendroglioma, ganglioglioma (neoplasm associated with chronic epilepsy in children and young adults and that may be associated with focal cortical dysplasia), DNET or pleomorphic xanthoastrocytoma. Hypothalamic hamartoma is another neoplasm that is typically associated with gelastic epilepsy in childhood. It usually has similar signal intensity to gray matter on all pulse sequences and typically does not enhance after administration of intravenous contrast. Epileptogenic hypothalamic hamartoma always affects the mammillary bodies and also often the tuber cinereum .
- 51. Left temporal low-grade glioma.
- 55. Dysembryoplastic neuroepithelial tumour (DNET).
- 56. Vascular malformations (VM). VM represent 5% of lesions found in series of patients with chronic epilepsy. Mainly arteriovenous malformations (AVMs) and cavernous malformations . To explain the seizures that occur in patients with AVMs two phenomena have been postulated: 1. Focal cerebral ischemia due to a steal phenomenon due to arteriovenous shunt. 2. Gliosis and hemosiderin deposits in the parenchyma due to subclinical bleeding. The sensitivity of MRI in detection is nearly 100%.
- 57. Left temporal cavernous malformation.
- 59. Gliosis / Miscellaneous. Gliosis is the end state of several injuries that can affect the central nervous system, mainly: trauma, infection and stroke. The findings are nonspecific at MRI although usually hyper-signal areas often are present in long TR sequences, associated with loss of volume sings (such as grooves widening and ventricular retraction) and encephalomaly areas. Emphasize the stroke as most common cause of epilepsy in the elderly. There are many other diseases that can cause seizures. -Parenchymal infectious processes (encephalitis, abscesses) with or without meningeal involvement: may present with seizures. - The Sturge-Weber syndrome or pial angiomatosis. Rasmussen's encephalitis: Childhood typical chronic encephalitis characterized by partial motor seizures and progressive cognitive and neurological deterioration; in image is characterized by a progressive unilateral cerebral cortical atrophy.