
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Article
- 1. ﻣﺠﻠﻪﻱ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ ﺍﻳﺮﺍﻥ ﺩﺍﻧﺸﮕﺎﻩ ﻋﻠﻮﻡ ﭘﺰﺷﻜﻲ ﻭ ﺧﺪﻣﺎﺕ ﺑﻬﺪﺍﺷﺘﻲ ـ ﺩﺭﻣﺎﻧﻲ ﺷﻬﻴﺪ ﺑﻬﺸﺘﻲ ﺩﻭﺭﻩﻱ ﺩﻭﺍﺯﺩﻫﻢ، ﺷﻤﺎﺭﻩﻱ ۴، ﺻﻔﺤﻪﻫﺎﻱ۰۰۴ ـ ۳۹۳ )ﺁﺑﺎﻥ ۹۸۳۱( ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ ﺩﺭ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻳﻲ ﻓﺎﺭﺱ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﻘﺎﻟﻪﻱ ﭘﮋﻭﻫﺸﻲ ﻣﺤﻠﻲ ﻭWHO ﺩﻛﺘﺮ ﺍﻣﻴﺮ ﺁﺩﻳﻨﻪﭘﻮﺭ۱، ﺩﻛﺘﺮ ﻣﻌﺼﻮﻣﻪ ﺗﻮﺣﻴﺪﻱ۱، ﺩﻛﺘﺮ ﻣﺤﻤﺪﺣﺴﻴﻦ ﺩﺑﺎﻍﻣﻨﺶ۱، ﺩﻛﺘﺮ ﭘﻴﻤﺎﻥ ﺟﻌﻔﺮﻱ۲، ﺩﻛﺘﺮ ۱ ﻣﺤﻤﺪﺭﺿﺎ ﻓﺘﺎﺣﻲ۳، ﺩﻛﺘﺮ ﻏﻼﻣﺤﺴﻴﻦ ﺭﻧﺠﺒﺮﻋﻤﺮﺍﻧﻲ ۱( ﻣﺮﮐﺰ ﺗﺤﻘﻴﻘﺎﺕ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ، ۲( ﺑﺨﺶ ﺁﻣﺎﺭ ﺯﻳﺴﺘﻲ ﻭ ۳( ﻣﺮﮐﺰ ﺗﺤﻘﻴﻘﺎﺕ ﮔﻮﺍﺭﺵ ﻭ ﮐﺒﺪ، ﺩﺍﻧﺸﮕﺎﻩ ﻋﻠﻮﻡ ﭘﺰﺷﮑﻲ ﺷﻴﺮﺍﺯ، ﻧﺸﺎﻧﻲ ﻣﮑﺎﺗﺒﻪﻱ ﻧﻮﻳﺴﻨﺪﻩﻱ ﻣﺴﺌﻮﻝ: ﺷﻴﺮﺍﺯ، ﺑﻴﻤﺎﺭﺳﺘﺎﻥ ﻧﻤﺎﺯﻱ، ﻣﺮﮐﺰ ﺗﺤﻘﻴﻘﺎﺕ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ، ﺻﻨﺪﻭﻕ ﭘﺴﺘﻲ: ۱۵۳۱۱-۷۳۹۱۷، ﺩﻛﺘﺮ ﻏﻼﻣﺤﺴﻴﻦ ﺭﻧﺠﺒﺮ ﻋﻤﺮﺍﻧﻲ؛ e-mail:hormone @ sums .ac .ir ﭼﻜﻴﺪﻩ ﻣﻘﺪﻣﻪ: ﺑﺘﺎﺯﮔﯽ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ )ﺍﺳﺘﺌﻮﭘﺮﻭﺯ( ﺑﻪ ﻋﻨﻮﺍﻥ ﻳﮏ ﻣﺸﮑﻞ ﺑﻬﺪﺍﺷﺘﻲ ﺍﺳﺎﺳﯽ ﺟﺎﻣﻌﻪ ﭘﺪﻳﺪ ﺁﻣﺪﻩ ﺍﺳﺖ. ﺍﻳﻦ ﺑﻴﻤﺎﺭﯼ ﺑﺎ ﮐﺎﻫﺶ ﻣﻴﺰﺍﻥ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻥ ﻫﻤﺮﺍﻩ ﺑﺎ ﺗﺨﺮﻳﺐ ﺭﻳﺰﺳﺎﺧﺘﺎﺭﻫﺎﻱ ﺑﺎﻓﺖ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﺸﺨﺺ ﻣﯽﺷﻮﺩ ﻭ ﻣﻮﺟﺐ ﺍﻓﺰﺍﻳﺶ ﺷﻜﺴﺘﮕﻲ ﻭ ﻧﺎﺗﻮﺍﻧﻲ، ﻫﻤﺮﺍﻩ ﺑﺎ ﻣﺮﮒ ﻭ ﻣﻴﺮ ﻣﯽﮔﺮﺩﺩ. ﻣﻮﺍﺩ ﻭ ﺭﻭﺵﻫﺎ: ﺩﺭ ﻳﮏ ﻣﻄﺎﻟﻌﻪﻱ ﻣﻘﻄﻌﻲ ۳۶۲ ﻣﺮﺩ ﺳﺎﻟﻢ ﺭﻭﺳﺘﺎﻳﻲ ﮐﻪ ﺩﺭ ﺳﻨﻴﻦ ۰۲ ﺗﺎ ۴۹ ﺳﺎﻝ ﺑﻮﺩﻧﺪ، ﺑﺮﺍﻱ ﺑﺮﺭﺳﻲ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺮﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﻭ ﺳﭙﺲ ﻣﻘﺎﻳﺴﻪﻱ ﺁﻥ ﺑﺎ ﻣﻌﻴﺎﺭﻫـﺎﻱ WHOﺍﻧﺘﺨﺎﺏ ﺷﺪﻧﺪ. ﺗﺮﺍﻛﻢ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ) (BMDﺑﻪ ﺭﻭﺵ DXAﺍﻧﺪﺍﺯﻩﮔﻴﺮﯼ ﺷﺪ. ﺍﺯ ﺭﻭﺵ ﺗﻄﺎﺑﻖ ﻣﻨﺤﻨﻲ ﺑﺮﺍﻱ ﺗﻌﻴﻴﻦ ﺳﻨﻲ ﮐﻪ ﺑﻴﺸﺘﺮﻳﻦ BMDﺩﺭ ﺁﻥ ﺍﻳﺠﺎﺩ ﻣﻲﺷﻮﻧﺪ ﻭ ﺍﺯ ﺁﻧﺎﻟﻴﺰ ﺭﮔﺮﺳﻴﻮﻥ ﺑﺮﺍﻱ ﺍﺭﺗﺒﺎﻁ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﻋﻮﺍﻣﻠﻲ ﹼ ﭼﻮﻥ ﺳﻦ ﻭ ﻧﻤﺎﻳﻪﻱ ﺗﻮﺩﻩﻱ ﺑﺪﻧﻲ ) (BMIﺍﺳﺘﻔﺎﺩﻩ ﺷﺪ. ﻳﺎﻓﺘﻪﻫﺎ: ﺑﻴﺸﺘﺮﻳﻦ BMDﺩﺭ ﺳﻨﻴﻦ ۰۲ ﺗﺎ ۴۲ ﺳﺎﻝ ﺍﻳﺠﺎﺩ ﻣﯽﺷﺪ.ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺑﺎﻻ ﺭﻓﺘﻦ ﺳﻦ ﺍﻓﺰﺍﻳﺶ ﻳﺎﻓﺖ، ﺑﺎ BMIﺍﺭﺗﺒﺎﻁ ﻣﻨﻔﻲ ﺩﺍﺷﺖ ﻭ ﺑﺮﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﻭ ﻣﺤﻠﻲ ﻣﺘﻔﺎﻭﺕ ﺑﻮﺩ. ﺷﻴﻮﻉ ﺁﻥ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ، ﮔﺮﺩﻥ ﻭ ﮐﻞ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺑﺎ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﺑﻪ ﺗﺮﺗﻴﺐ ۸/۳%، ۸/۴۲% ﻭ ۸/۴۱% ﻭ ﺍﻳﻦ ﻣﻘﺪﺍﺭﻫﺎ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭ WHOﺑﻪ ﺗﺮﺗﻴﺐ ۰۱% ﻭ ۱/۶% ﻭ ۴۲% ﺑﻮﺩ. ﻧﺘﻴﺠﻪﮔﻴﺮﻱ: ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﻳﺎ ﻣﻌﻴﺎﺭﻫﺎﻱ WHO ﺑﺮﺍﻱ ﺑﺮﺭﺳﻲ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ، ﻣﻲﺗﻮﺍﻧﺪ ﻳﺎﻓﺘﻪﻫﺎﻱ ﻣﺘﻔﺎﻭﺗﻲ ﺩﺭ ﺯﻣﻴﻨﻪﻱ ﺷﻴﻮﻉ ﻣﻮﺍﺭﺩ ﺍﻳﻦ ﺑﻴﻤﺎﺭﻱ ﺍﺭﺍﻳﻪ ﺩﻫﺪ، ﺑﻨﺎﺑﺮﺍﻳﻦ ﺑﺮﺭﺳﻲﻫﺎﻱ ﺁﻳﻨﺪﻩﻧﮕﺮ ﺩﺭ ﻣﻮﺭﺩ ﺭﺍﺑﻄﻪﻱ ﺍﺣﺘﻤﺎﻝ ﺷﮑﺴﺘﮕﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺩﻭ ﻣﻌﻴﺎﺭ ﻧﺎﻣﺒﺮﺩﻩ ﺗﻮﺻﻴﻪ ﻣﻲﺷﻮﺩ. ﻭﺍﮊﮔﺎﻥ ﻛﻠﻴﺪﻱ: ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ، ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻥ، ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ، WHO ﺩﺭﻳﺎﻓﺖ ﻣﻘﺎﻟﻪ: ۰۲/۲۱/۸۸ ـ ﺩﺭﻳﺎﻓﺖ ﺍﺻﻼﺣﻴﻪ: ۸/۳/۹۸ ـ ﭘﺬﻳﺮﺵ ﻣﻘﺎﻟﻪ: ۳۱/۴/۹۸ ﻫﻴﭻ ﻋﻼﻣﺘﻲ ﭘﻴﺸﺮﻓﺖ ﻣﻲﻛﻨﺪ ﺗﺎ ﺑﺎ ﺍﻧﺪﻙ ﻓﻌﺎﻟﻴﺖ، ﺷﻜﺴﺘﮕﻲ ﻣﻘﺪﻣﻪ ۲،۱ ﺍﺗﻔﺎﻕ ﺑﻴﻔﺘﺪ. ﺩﺭ ﺁﻣﺮﻳﻜﺎ ۲۱ ﻣﻴﻠﻴﻮﻥ ﻣﺮﺩ ﻭ ﺯﻥ ﺑﻪ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﺒﺘﻼ ﺑﻴﻤﺎﺭﻱ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ iﻳﺎ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺷﺎﻳﻊﺗﺮﻳﻦ ﺑﻴﻤﺎﺭﻱ ﻫﺴﺘﻨﺪ ﻭ ﺣﺪﺍﻗﻞ ۰۴ ﻣﻴﻠﻴﻮﻥ ﻧﻔﺮ ﮐﺎﻫﺶ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﺘﺎﺑﻮﻟﻴﻚ ﺍﺳﺘﺨﻮﺍﻥ ﺍﺳﺖ ﻛﻪ ﻣﻲﺗﻮﺍﻧﺪ ﺑﺎﻋﺚ ﻛﺎﻫﺶ ﺍﺳﺘﺤﻜﺎﻡ )ﺍﺳﺘﺌﻮﭘﻨﻲ( ﺩﺍﺭﻧﺪ.۲ ﺷﻴﻮﻉ ﺍﻳﻦ ﺑﻴﻤﺎﺭﻱ ﺑﺎ ﺍﻓﺰﺍﻳﺶ ﺳﻦ، ﺯﻳﺎﺩ ﺍﺳﺘﺨﻮﺍﻥ ﻭ ﺩﺭﻧﺘﻴﺠﻪ ﺍﻓﺰﺍﻳﺶ ﺧﻄﺮ ﺷﻜﺴﺘﮕﻲ ﺷﻮﺩ. ﺍﻳﻦ ﻣﻲﺷﻮﺩ ﻣﺮﺩﺍﻥ ﻧﺴﺒﺖ ﺑﻪ ﺯﻧﺎﻥ ﻛﻤﺘﺮ ﻣﺒﺘﻼ ﻣﻲﺷﻮﻧﺪ. ﻣﺮﺩﺍﻥ، ﺑﻴﻤﺎﺭﻱ ﺑﻪ ﻋﻨﻮﺍﻥ ﻳﻚ ﺑﻴﻤﺎﺭﻱ ﺧﺎﻣﻮﺵ ﺷﻨﺎﺧﺘﻪ ﺷﺪﻩ، ﻛﻪ ﺑﺪﻭﻥ ﺩﺍﺭﺍﻱ ﺗﻮﺩﻩﻱ ﺍﺳﻜﻠﺘﻲ ﺑﻴﺸﺘﺮﻱ ﻫﺴﺘﻨﺪ ﻭ ﺗﻐﻴﻴﺮﻫﺎﻱ ﻫﻮﺭﻣﻮﻧﻲ i- Osteoporosis
- 2. ﺩﻭﺭﻩﻱ ﺩﻭﺍﺯﺩﻫﻢ, ﺷﻤﺎﺭﻩﻱ ۴، ﺁﺑﺎﻥ ۹۸۳۱ ﻣﺠﻠﻪﻱ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ ﺍﻳﺮﺍﻥ ۴۹۳ ﺭﻭﺳﺘﺎﻳﻲ ﺑﺮ ﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﻭ ﺳﭙﺲ ﺷﻴﻮﻉ ﺁﻥ ﺭﺍ ﺑﺎ ﮐﻪ ﻣﻮﺟﺐ ﺗﺤﻠﻴﻞ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﻲﺷﻮﺩ، ﺩﺭ ﺁﻧﻬﺎ ﺗﺪﺭﻳﺠﻲ ۴،۳ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻴﺰﺍﻥ ) ،ii(PBMﺑﺮﺍﺳﺎﺱ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﺑﺮﺭﺳﻲ ﺑﺎ ﺍﻳﻦ ﺣﺎﻝ ﺩﺭ ﻣﺮﺩﺍﻥ ﺑﺮﺍﻱ ﻫﺮﻣﻘﺪﺍﺭ ﻭ ﺧﻔﻴﻒ ﻣﻲﺑﺎﺷﺪ. ﻛﻨﻴﻢ. ﺍﻧﺤﺮﺍﻑ ﻣﻌﻴﺎﺭ ﻛﺎﻫﺶ ﺩﺭ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻥ ﺍﺣﺘﻤﺎﻝ ﺷﻜﺴﺘﮕﻲ ﻭ ۶-۴ ﻣﻮﺍﺩ ﻭ ﺭﻭﺵﻫﺎ ﻣﺮﮒ ﻭ ﻣﻴﺮ ﺑﻴﺸﺘﺮ ﺍﺯ ﺯﻧﺎﻥ ﺍﺳﺖ. ﺑﺎ ﺗﻮﺟﻪ ﺑﻪ ﺗﻔﺎﻭﺕﻫﺎﻳﻲ ﮐﻪ ﺩﺭ ﮊﻧﺘﻴﮏ، ﺷﻴﻮﻩﻱ ﺯﻧﺪﮔﻲ، ﻧﻮﻉ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﺍﺯ ﻧﻮﻉ ﻣﻘﻄﻌﻲ- ﺗﻮﺻﻴﻔﻲ ﺑﻮﺩ ﻭ ﺩﺭ ﺳﺎﻝﻫﺎﻱ ﺗﻐﺬﻳﻪ ﻭ ﻓﻌﺎﻟﻴﺖ ﺩﺭ ﺟﺎﻣﻌﻪﻫﺎﻱ ﻣﺨﺘﻠﻒ ﻭﺟﻮﺩ ﺩﺍﺭﺩ، ﺗﻮﺩﻩﻱ ۸۸-۷۸۳۱ ﺍﻧﺠﺎﻡ ﺷﺪ. ﺍﻳﻦ ﺑﺮﺭﺳﻲ ﻗﺴﻤﺘﻲ ﺍﺯ ﻣﻄﺎﻟﻌﻪﻱ ﮐﻮﺍﺭ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻭ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﻲﺗﻮﺍﻧﺪ ﺑﺎ ) (kavar cohortﺑﻮﺩ ﺣﺠﻢ ﻧﻤﻮﻧﻪ ﺷﺎﻣﻞ ۰۰۴۶ ﻓﺮﺩ ﺭﻭﺳﺘﺎﻳﻲ ﻣﻌﻴﺎﺭ WHOﮐﻪ ﺍﺯ ﺟﻤﻌﻴﺖ ﺳﺎﻟﻢ ﺁﻣﺮﻳﮑﺎ ﮔﺮﻓﺘﻪ ﺷﺪﻩ، ﻣﺘﻔﺎﻭﺕ ﺳﺎﻛﻦ ﺩﺭ ﻣﻨﻄﻘﻪﻱ ﮐﻮﺍﺭ ﺍﺳﺘﺎﻥ ﻓﺎﺭﺱ ﺍﻳﺮﺍﻥ ﺑﻮﺩﻧﺪ. ﺍﻳﻦ ﻣﻨﻄﻘﻪ ﺑﺎﺷﺪ. ﺩﺭ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ ﻣﺨﺘﻠﻒ، ﺷﻴﻮﻉ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺩﺭ ﻣﺮﮐﺰ ﺍﺳﺘﺎﻥ ﻓﺎﺭﺱ ﺩﺭ ۵۴ ﮐﻴﻠﻮﻣﺘﺮﻱ ﺷﻬﺮ ﺷﻴﺮﺍﺯ ﻗﺮﺍﺭ ﺟﺎﻣﻌﻪﻫﺎﻱ ﺷﻬﺮﻱ ﻳﺎ ﺭﻭﺳﺘﺎﻳﻲ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭ WHOﻭ ﮔﺮﻓﺘﻪ ﻭ ﺁﺏ ﻭ ﻫﻮﺍﻳﻲ ﻣﺎﻧﻨﺪ ﺷﻬﺮ ﺷﻴﺮﺍﺯ ﺩﺍﺭﺩ. ﺑﻴﺸﺘﺮ ﻣﺮﺩﺍﻥ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﺁﺯﻣﻮﺩﻩ ﺷﺪﻩ ﺍﺳﺖ. ﺩﺭ ﺷﻴﺮﺍﺯ ﻣﻄﺎﻟﻌﻪﺍﻱ ﺗﻮﺳﻂ ﺭﻭﺳﺘﺎﻳﻲ ﺍﻳﻦ ﻣﻨﻄﻘﻪ ﮐﺸﺎﻭﺭﺯ ﻫﺴﺘﻨﺪ. ﺟﻤﻌﻴﺖ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ، ﺩﻛﺘﺮ ﻋﻤﺮﺍﻧﻲ ﻭ ﻫﻤﻜﺎﺭﺍﻥ ﺍﻧﺠﺎﻡ ﺷﺪ ﻛﻪ ﺷﻴﻮﻉ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﺮﺩﺍﻧﻲ ﺑﻮﺩﻧﺪ ﮐﻪ ﺳﻦ ۰۲ ﺳﺎﻝ ﻳﺎ ﺑﺎﻻﺗﺮ ﺩﺍﺷﺘﻪ، ﺳﺎﻛﻦ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﻣﺮﺩﺍﻥ ﺷﻴﺮﺍﺯﻱ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻘﻴﺎﺱ WHO ﺭﻭﺳﺘﺎﻫﺎﻱ ﺑﺨﺶ ﻛﻮﺍﺭ ﺑﻮﺩﻧﺪ ﻭ ﺣﺪﺍﻗﻞ ۵ ﺳﺎﻝ ﺩﺭ ﺁﻥ ﻣﻨﻄﻘﻪ ۴/۶۱% ﻭ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ۴/۳۱% ﺑﻮﺩ.۷ ﺩﺭ ﻣﻄﺎﻟﻌﻪﻱ ﺯﻧﺪﮔﻲ ﻛﺮﺩﻩ ﺑﻮﺩﻧﺪ. ﺣﺠﻢ ﻧﻤﻮﻧﻪ ﺩﺭ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﺑﺮ ﺍﺳﺎﺱ ﭼﻨﺪ ﻣﺮﮐﺰﻱ ﺍﻳﺮﺍﻥ ) i(IMOSﻧﺸﺎﻥ ﺩﺍﺩﻩ ﺷﺪ ﻛﻪ ﺷﻴﻮﻉ ﮐﻠﻲ 2 Z 2α / 2 × δ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻭ ﺍﺳﺘﺌﻮﭘﻨﻲ ﺩﺭ ﻣﺮﺩﺍﻥ ﺑﺎﻻﻱ ۰۵ ﺳﺎﻝ ﺍﻳﺮﺍﻧﻲ، = nﻭ ﺍﻧﺤﺮﺍﻑ ﻣﻌﻴﺎﺭ ۱۱/۰، ۲۱/۰، 2 ﻓﺮﻣﻮﻝ d ۰۵% ﺍﺳﺖ ﻭ ۳۱% ﺍﺯ ﻣﺮﺩﺍﻥ ﺩﺭ ﻣﻌﺮﺽ ﺧﻄﺮ ﺷﻜﺴﺘﮕﻲ ﻫﺴﺘﻨﺪ. ۲۱/۰، ۱۱/۰، ۳۱/۰ ﻭ ۱۱/۰ ﺑﺪﺳﺖ ﺁﻣﺪ. ﺍﻳﻦ ﺣﺠﻢ ﺑﻪ ﺗﺮﺗﻴﺐ ﺷﻴﻮﻉ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﻣﺮﺩﺍﻥ ﺑﺎﻻﺗﺮ ﺍﺯ ۰۵ ﺑﺮﺍﻱ ﮔﺮﻭﻩﻫﺎﻱ ﺳﻨﻲ ﻣﺨﺘﻠﻒ ﻣﺮﺩﺍﻥ ﺑﻪ ﺷﺮﺡ ﺯﻳﺮ ﺑﻮﺩ: ﻣﺮﺩﺍﻥ ﺳﺎﻝ ﺑﺮﺍﺳﺎﺱ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﻭ IMOSﺑﻪ ﺗﺮﺗﻴﺐ،۳% ﻭ ۰۲-۹۲ ﺳﺎﻟﻪ ۵۳ ﻧﻔﺮ، ﻣﺮﺩﺍﻥ ۰۳-۹۳ ﺳﺎﻟﻪ ۰۳ ﻧﻔﺮ، ﻣﺮﺩﺍﻥ ۰۴- ۷/۲% ﺑﻮﺩ ﻛﻪ ﺍﻳﻦ ﻣﻘﺪﺍﺭ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﮐﻤﺮ ﺑﻪ ﺗﺮﺗﻴﺐ ۲/۴۱% ﻭ ۹۴ ﺳﺎﻟﻪ ۰۳ ﻧﻔﺮ، ﻣﺮﺩﺍﻥ ۰۵-۹۵ ﺳﺎﻟﻪ ۰۴ ﻧﻔﺮ ﻭ ﻣﺮﺩﺍﻥ ۰۶ ۵/۳% ﺑﻪ ﺩﺳﺖ ﺁﻣﺪ.۸ ﻫﻢﭼﻨﻴﻦ، ﺩﺭ ﻣﻄﺎﻟﻌﻪﺍﻱ ﮐﻪ ﺩﺭ ﭼﻴﻦ ﺍﻧﺠﺎﻡ ﺳﺎﻟﻪ ﻳﺎ ﻣﺴﻦﺗﺮ ﺑﺮﺍﺑﺮ ۰۳ ﻧﻔﺮ ﺗﻌﻴﻴﻦ ﺷﺪ ﻛﻪ ﺩﺭ ﻫﺮ ﺩﻫﮏ ﺣﺪﺍﻗﻞ ﮔﺮﻓﺖ ﺑﺮﺍﺳﺎﺱ ﺑﺮﻃﺒﻖ ﻣﻌﻴﺎﺭﻫﺎﻱ ﭼﻴﻨﻲ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ ﺩﺭ ۰۶ ﻧﻔﺮ ﺍﻧﺘﺨﺎﺏ ﺷﺪﻧﺪ. ﻧﻤﻮﻧﻪﮔﻴﺮﻱ ﺑﻪ ﺭﻭﺵ ﺳﻴﺴﺘﻤﻲ ﺗﺼﺎﺩﻓﻲ ﮔﺮﺩﻥ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ۹۰۱% ﺑﻴﺸﺘﺮ ﺍﺯ ﺷﻴﻮﻉ ﺁﻥ ﺑﺮﺍﺳﺎﺱ ﺑﻮﺩ. ﺑﺮﺍﺳﺎﺱ ﺷﻤﺎﺭﻩﻱ ﭘﺮﻭﻧﺪﻩﻱ ﺧﺎﻧﻮﺍﺭ ﺭﻭﺳﺘﺎﻳﻲ ۰۰۳ ﻧﻔﺮ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﺑﻮﺩ. ﺍﻳﻦ ﻳﺎﻓﺘﻪﻫﺎ ﻭ ﻳﺎﻓﺘﻪﻫﺎﻱ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ ﺍﻧﺘﺨﺎﺏ ﺷﺪﻧﺪ ﻭ ﺩﺭ ﭘﺎﻳﺎﻥ ﺗﺤﻠﻴﻞ ﻧﻬﺎﻳﻲ ﺩﺭ ۳۶۲ ﻧﻔﺮ ﺍﺯ ﻣﺮﺩﺍﻥ ﻣﺸﺎﺑﻪ ﻧﺸﺎﻥﺩﻫﻨﺪﻩﻱ ﺗﻔﺎﻭﺕ ﺁﺷﮑﺎﺭ ﻣﻌﻴﺎﺭ WHOﺑﺎ ﻣﻌﻴﺎﺭ ﺩﺍﺭﺍﻱ ﺷﺮﺍﻳﻂ ﺍﻧﺠﺎﻡ ﺷﺪ. ﻣﺮﺩﺍﻧﻲ ﻛﻪ ﻓﻌﺎﻟﻴﺖ ﻓﻴﺰﻳﻜﻲ ﭼﻨﺪﺍﻧﻲ ۰۱،۹ ﻣﺤﻠﻲ ﺍﺳﺖ. ﻧﺪﺍﺷﺘﻨﺪ، ﺳﺎﺑﻘﻪﻱ ﺷﮑﺴﺘﮕﻲ ﻳﺎ ﺑﻴﻤﺎﺭﻱ ﺳﻴﺴﺘﻤﻲ ﺍﺯ ﻗﺒﻴﻞ ﺟﻤﻌﻴﺖﻫﺎﻱ ﺷﻬﺮﻱ ﻭ ﺭﻭﺳﺘﺎﻳﻲ ﻧﻴﺰ ﺍﺯ ﻧﻈﺮ ﺷﻴﻮﻉ ﭘﻮﻛﻲ ﻧﺎﺭﺳﺎﻳﻲ ﻣﺰﻣﻦ ﻛﻠﻴﻪ، ﻛﺒﺪ، ﻗﻠﺐ ﻭ ﺭﻳﻪ، ﻫﻤﻮﮔﻠﻮﺑﻴﻨﻮﭘﺎﺗﻲ، ﺍﺳﺘﺨﻮﺍﻥ ﺑﺮﺭﺳﻲ ﺷﺪﻩﺍﻧﺪ. ﻛﻪ ﺩﺭ ﺑﻌﻀﻲ ﻣﻄﺎﻟﻌﻪﻫﺎ ﺩﻳﺪﻩ ﺭﻭﻣﺎﺗﻴﺴﻢ ﻣﻔﺼﻠﻲ، ﺳﺮﻃﺎﻥﻫﺎ ﻭ ﺑﻴﻤﺎﺭﻱﻫﺎﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﻴﺰﺍﻥ ﺷﻜﺴﺘﮕﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﻭ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺷﻨﺎﺧﺘﻪ ﺷﺪﻩ ﺩﺍﺷﺘﻨﺪ، ﺍﺯ ﻣﻄﺎﻟﻌﻪ ﺧﺎﺭﺝ ﻭ ﭘﺲ ﺍﺯ ﺑﺮﺭﺳﻲﻫﺎﻱ ﺟﺎﻣﻌﻪﻫﺎﻱ ﺭﻭﺳﺘﺎﻳﻲ ﻛﻤﺘﺮ ﺍﺯ ﺷﻬﺮﻱ ﺍﺳﺖ ﻭ ﺩﺭ ﺳﺎﻳﺮ ﻻﺯﻡ ﺍﻓﺮﺍﺩﻱ ﺑﺎ ﻇﺎﻫﺮ ﺳﺎﻟﻢ ﺍﻧﺘﺨﺎﺏ ﺷﺪﻧﺪ. ﺍﻳﻦ ﭘﮋﻭﻫﺶ ﺍﺯ ﻧﻈﺮ ﻣﻄﺎﻟﻌﻪﻫﺎ ﺷﮑﺴﺘﮕﻲ ﻭ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺭﻭﺳﺘﺎﻫﺎ ﺷﺎﻳﻊﺗﺮ ﻣﻌﻴﺎﺭﻫﺎﻱ ﺍﺧﻼﻕ ﭘﺰﺷﮑﻲ ﺗﻮﺳﻂ ﮐﻤﻴﺘﻪﻱ ﻣﺮﺑﻮﻁ ﺩﺭ ﺩﺍﻧﺸﮕﺎﻩ ۱۱ ﻭﺩﺭ ﭼﻨﺪ ﺑﺮﺭﺳﻲ ﺑﺪﻭﻥ ﺗﻔﺎﻭﺕ ﺑﻮﺩﻩﺍﺳﺖ. ﻋﻠﻮﻡ ﭘﺰﺷﮑﻲ ﺷﻴﺮﺍﺯ ﺗﺄﻳﻴﺪ ﺷﺪ. ﻫﻢﭼﻨﻴﻦ ﻓﺸﺎﺭﺧﻮﻥ، ﻗﺪ ﻭ ﻭﺯﻥ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ ﺍﻧﺠﺎﻡ ﺷﺪﻩ ﺩﺭ ﻣﻮﺭﺩ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺳﻄﺢ ﺍﻧﺠﺎﻡ ﮔﺮﻓﺖ ﻭ ﻣﻘﺪﺍﺭ ﻧﻤﺎﻳﻪﻱ ﺗﻮﺩﻩﻱ ﺑﺪﻥ ) iii(BMIﻣﺤﺎﺳﺒﻪ ﺭﻭﺳﺘﺎﻫﺎ ﺑﻪ ﻭﻳﮋﻩ ﺩﺭ ﻣﺮﺩﺍﻥ ﺑﺴﻴﺎﺭ ﻣﺤﺪﻭﺩ ﺍﺳﺖ ﻭ ﺍﻳﻦ ﺷﺪ. ﺑﺮﺭﺳﻲﻫﺎ ﺗﺎﮐﻨﻮﻥ ﺩﺭ ﺳﻄﺢ ﮐﺸﻮﺭﻱ ﺍﻧﺠﺎﻡ ﻧﺸﺪﻩ، ﻳﺎ ﮔﺰﺍﺭﺷﻲ ﺍﺯ ﺁﻥﻫﺎ ﺩﺭ ﺩﺳﺘﺮﺱ ﻧﻤﻲﺑﺎﺷﺪ. ﺑﻨﺎﺑﺮﺍﻳﻦ، ﺑﺎ ﺗﻮﺟﻪ ﺑﻪ ﻧﮑﺎﺕ ﺫﮐﺮ ﺷﺪﻩ ﺩﺭﺻﺪﺩ ﺑﺮﺁﻣﺪﻳﻢ ﺷﻴﻮﻉ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍ ﺩﺭ ﻣﺮﺩﺍﻥ ii - Peak Bone Mass iii - Body Mass Index i- Iranian Multi Center Osteoporosis Study
- 3. ۵۹۳ ﺍﻭﺳﺘﺌﻮﭘﺮﻭﺯ ﺩﺭ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻫﺎﻱ ﻓﺎﺭﺱ ﺩﻛﺘﺮ ﺍﻣﻴﺮ ﺁﺩﻳﻨﻪﭘﻮﺭ ﻭ ﻫﻤﻜﺎﺭﺍﻥ ﺟﺪﻭﻝ ۱ـ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺗﻦﺳﻨﺠﻲ ﺍﻓﺮﺍﺩ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﺳﻨﺠﺶ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻥ ﺑﻪ ﺭﻭﺵ ) i(DEXAﺑﺎ ﺍﺳﺘﻔـﺎﺩﻩ ﻧﻤﺎﻳﻪﻱ ﺗﻮﺩﻩﻱ ﻗﺪ ﻭﺯﻥ ﺗﻌﺪﺍﺩ ﮔﺮﻭﻩ ﺍﺯ ﺩﺳﺘﮕـﺎﻩ ﻟﻮﻧﺎﺭ ) (DPX-IQ, Lunar Co., Madison, WIﺩﺭ † * ﺑﺪﻥ)ﻛﻴﻠﻮﮔﺮﻡ ﺑﺮ )ﺳﺎﻧﺘﻲﻣﺘﺮ( )ﻛﻴﻠﻮﮔﺮﻡ( ﺳﻨﻲ ‡ ﺍﺳﺘﺨﻮﺍﻥﻫﺎﻱ ﺭﺍﻥ )ﮔﺮﺩﻥ ﻭ ﻛﻞ ﺍﺳﺘﺨﻮﺍﻥ( ﻭﻧﻤﺎﻱ ﻗﺪﺍﻣﻲ- ﻣﺘﺮﻣﺮﺑﻊ( )ﺳﺎﻝ( ﺧﻠﻔﻲ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﺍﻓﺮﺍﺩ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﻭ ﻣﻴﺰﺍﻥ ) BMDﮔﺮﻡ ۳±۲۲ ۷±۳۷۱ ۹±۹۶ ۰۵ ۹۲-۰۲ ۴±۳۲ ۸±۹۶۱ ۲۱±۶۶ ۱۵ ۹۳-۰۳ ﺑﺮ ﺳﺎﻧﺘﻲﻣﺘﺮ ﻣﺮﺑﻊ( ﻭ ) iiBMCﮔﺮﻡ( ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﻭ ۴±۴۲ ۷±۸۶۱ ۲۱±۹۶ ۷۵ ۹۴-۰۴ T-scoreﻭ Z-scoreﺑﺮﺍﺳﺎﺱ ﻣﻌﻴﺎﺭﻫﺎﻱ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ، ۳±۳۲ ۶±۷۶۱ ۱۱±۶۶ ۲۵ ۹۵-۰۵ WHOﺍﻧﺪﺍﺯﻩﮔﻴﺮﻱ ﺷﺪﻧﺪ. ﮐﺎﻟﻴﺒﺮﻩ ﻛﺮﺩﻥ ﺩﺳﺘﮕﺎﻩ ﺑﻪ ﺻﻮﺭﺕ ۳±۳۲ ۷±۵۶۱ ۰۱±۲۶ ۲۵ ۰۶ ≥ ﺭﻭﺯﺍﻧﻪ ﻭ ﺍﻧﺪﺍﺯﻩﮔﻴﺮﻱﻫﺎ ﺗﻮﺳﻂ ﻳﮏ ﺩﺳﺘﮕﺎﻩ ﻭ ﻳﮏ ﻓﺮﺩ ۴±۳۲ ۷±۸۶۱ ۱۱±۵۶ ۲۶۲ ﮐﻞ ﮐﻤﺘﺮ ﺍﺯ ۱/۱% ﺁﻣﻮﺯﺵﺩﻳﺪﻩ ﺍﻧﺠﺎﻡ ﺷﺪ. ﺣﺴﺎﺳﻴﺖ ﺩﺳﺘﮕﺎﻩ iii * ﺍﻋﺪﺍﺩ ﺑﻪ ﺻﻮﺭﺕ ﻣﻴﺎﻧﮕﻴﻦ±ﺍﻧﺤﺮﺍﻑ ﻣﻌﻴﺎﺭ ﺑﻴﺎﻥ ﺷﺪﻩﺍﻧﺪ. ﺑﻮﺩ. ﭘﺲ ﺍﺯ ﻣﺤﺎﺳﺒﻪﻱ ،PBMﻣﻘﺪﺍﺭ ) (T-scoreﺑﺮﺍﺳﺎﺱ ﺑﻴﺸﺘﺮﻳﻦ ﻣﻘﺪﺍﺭ BMDﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ، ﮔﺮﺩﻥ ﺭﺍﻥ ﻭ ﮐﻞ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﺑﻪ ﺩﺳﺖ ﺁﻣﺪ. ﺍﻃﻼﻋﺎﺕ ﺑﻪ ﺩﺳﺖ ﺁﻣﺪﻩ ﺑﺎ ﺭﺍﻥ ) (Total femur/Hipﺩﺭ ﮔﺮﻭﻩ ﺳﻨﻲ ۹۲-۰۲ ﺳﺎﻝ ﺩﻳﺪﻩ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻧﺮﻡﺍﻓﺰﺍﺭ SPSSﻧﺴﺨﻪﻱ ۵۱ ﺟﻤﻊﺁﻭﺭﻱ ﻭ ﺁﻧﺎﻟﻴﺰ ﺷﺪ. ﻭ ﻣﻘﺪﺍﺭ BMDﺍﻳﻦ ﻣﻨﺎﻃﻖ ﺑﺎ ﺍﻓﺰﺍﻳﺶ ﺳﻦ ﺑﻪ ﻃﻮﺭ ﺷﺪ. ﻣﻌﻨﻲﺩﺍﺭﻱ ﮐﻢ ﺷﺪ ) ۱۰۰/۰< .(Pﻫﻢﭼﻨﻴﻦ، BMCﺩﺭ ﮔﺮﻭﻩﻫﺎﻱ ﺍﺯ ﺁﺯﻣﻮﻥ ﺗﺤﻠﻴﻞ ﺭﮔﺮﺍﺳﻴﻮﻥ ﺑﺮﺍﻱ ﺑﺮﺭﺳﻲ ﺍﺛﺮﻫﺎﻱ ﻣﺴﺘﻘﻞ ﻣﺨﺘﻠﻒ ﺳﻨﻲ ﺗﻔﺎﻭﺕ ﺩﺍﺷﺖ ﻭ ﺑﺎ ﺍﻓﺰﺍﻳﺶ ﺳﻦ ﺑﻄﻮﺭ ﻭﺍﺿﺤﻲ BMIﻭ ﺳﻦ ﺑﺮ ﺷﻴﻮﻉ ﭘﻮﻛﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺍﺳﺘﻔﺎﺩﻩ ﺷﺪ. ﮐﻢ ﺷﺪ. ) ۱۰۰/۰< .(Pﻣﻘﺪﺍﺭ ﻭ ﺯﻣﺎﻥ ﺍﻳﺠـﺎﺩ PBMﺗﻮﺳــﻂ ﺍﺯ ﺭﻭﺵ Fit Curveﺑﺮﺍﻱ ﺗﻌﻴﻴﻦ ﺳﻨﻲ ﮐﻪ PBMﺩﺭ ﺁﻥ ﹼ ﺭﻭﺵ Regression equationﺗﻌﻴﻴـﻦ ﮔﺮﺩﻳــﺪ )ﺟـﺪﻭﻝ ۲(. ﺍﻳﺠﺎﺩ ﺷﺪ، ﺍﺳﺘﻔﺎﺩﻩ ﮔﺮﺩﻳﺪ. ﻫﻤﺎﻥﻃﻮﺭ ﮐﻪ ﮔﻔﺘﻪ ﺷﺪ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﻣﻴﺎﻧﮕﻴﻦ BMDﮔﺮﻭﻩ ﻣﺮﺟﻊ ﺑﻪ ﻋﻨﻮﺍﻥ )ﻣﻘﺪﺍﺭ ﻣﺮﺟﻊ( ﺩﺭ ﻧﻈﺮ ﺍﺯ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺑﺎﻻ ﻭ ﻓﺮﻣﻮﻝ ﺯﻳﺮ T-scoreﻣﺤﻠﻲ )ﻣﻌﻴﺎﺭ ﺍﻳﺮﺍﻧﻲ( ﮔﺮﻓﺘﻪ ﻭ ﻣﺤﺎﺳﺒﻪ ﺷﺪ )ﺟﺪﻭﻝ ۳(. ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻘﺎﺩﻳﺮ PBM ﺑﻪ ﺩﺳﺖ ﺁﻣﺪ. ﺍﺳﺘﺎﻧﺪﺍﺭﺩ ﺩﺳﺘﮕﺎﻩ، ﻣﻴﺎﻧﮕﻴﻦ PBMﺟﻤﻌﻴﺖ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﺑﺎ ﺗﺮﺍﮐﻢ ﺍﺳﺘﺨﻮﺍﻥ ﻓﺮﺩ ﻣﻮﺭﺩ ﻧﻈﺮ - ﻣﻴﺎﻧﮕﻴﻦ ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﮐﻢ ﺩﺭ ﮔﺮﻭﻩ ﻣﺮﺟﻊ ۲۱،۷ = T-score ﻣﻘﺎﺩﻳﺮ ﺍﺳﺘﺎﻧﺪﺍﺭﺩ ﻣﻘﺎﻳﺴﻪ ﺷﺪ. ﺍﻧﺤﺮﺍﻑ ﻣﻌﻴﺎﺭ ﻣﻴﺎﻧﮕﻴﻦ ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﮐﻢ ﺩﺭ ﮔﺮﻭﻩ ﻣﺮﺟﻊ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﻨﻲ ﻭ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺍﻓﺮﺍﺩ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﺑﺮﺍﻱ ﻣﻘﺎﻳﺴﻪﻱ ﻣﻴﺎﻧﮕﻴﻦ PBMﺑﺎ ﻣﻘﺪﺍﺭﻫﺎﻱ ﺍﺳﺘﺎﻧﺪﺍﺭﺩ ﺑﺮﺍﺳﺎﺱ T-scoreﺁﻣﺮﻳﮑﺎ )ﮐﻪ ﺩﺭ ﺩﺳﺘﮕﺎﻩﻫﺎﻱ BMDﺑﻪ ﻃﻮﺭ ﺩﺳﺘﮕﺎﻩ ﺍﺯ ﻧﺮﻡﺍﻓﺰﺍﺭ ﺪ ﻛﻠﻚ ) (med calcﻧﺴﺨﻪﻱ ۰/۰/۲/۰۱ ﻣ ﻣﻌﻤﻮﻝ ﺍﺳﺘﻔﺎﺩﻩ ﻣﻲﺷﻮﺩ( ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﺑﻪ ﺗﺮﺗﻴﺐ ۲۴% ﻃﺒﻖ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﻭ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ، ۲۱،۷ ﺍﺳﺘﻔﺎﺩﻩ ﺷﺪ. ﻭ۴۲%، ﺩﺭ ﮔﺮﺩﻥ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺑﻪ ﺗﺮﺗﻴﺐ ۶۴% ﻭ ۰۱%، ﻭ ﺩﺭ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﻪ ﺻﻮﺭﺕ T-Scoreﮐﻤﺘﺮ ﻳﺎ ﻣﺴﺎﻭﻱ ۵/۲- ﻭ ﻛﻞ ﺭﺍﻥ ﺑﻪ ﺗﺮﺗﻴﺐ ۸۴% ﻭ ۶% ﺑﻮﺩ. ﭘﺲ ﺍﺯ ﺗﻌﻴﻴﻦ ،PBMﻣﻘﺪﺍﺭ ﻛﺎﻫﺶ ﺗﺮﺍﻛﻢ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻳﺎ ﺍﺳﺘﺌﻮﭘﻨــﻲ ﺑﻪ ﺻـــﻮﺭﺕ T-Scoreﻣﺤﻠﻲ ﺑﻪ ﺩﺳﺖ ﺁﻣﺪ ﻭ ﻣﺠﺪﺩﹰﺍ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﻨﻲ ﻭ -۱ T-Scoreﺗﺎ ۵/۲-ﻭ ﺍﻓﺮﺍﺩ ﺑﺎ T-Scoreﺑﻴﺸﺘﺮ ﺍﺯ ۱- ﺳﺎﻟﻢ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﺤﺎﺳﺒﻪ ﺷﺪ. ﺩﺭ ﻧﻈﺮ ﮔﺮﻓﺘﻪ ﺷﺪﻧﺪ ﻭ ﺑﺮﺭﺳﻲﻫﺎﻱ ﻻﺯﻡ ﺍﻧﺠﺎﻡ ﺷﺪ. ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺍﻓﺰﺍﻳﺶ ﺳﻦ ﺑﻴﺸﺘﺮ ﻭ ﺑﺎ ﺍﻓﺰﺍﻳﺶ BMIﮐﻤﺘﺮ ﺷﺪ ﻭ ﺍﻳﻦ ﺍﺭﺗﺒﺎﻁ ﺍﺯ ﻧﻈﺮ ﺁﻣﺎﺭﻱ ﻣﻌﻨﻲﺩﺍﺭ ﻳﺎﻓﺘﻪﻫﺎ ﺑﻮﺩ. )۱۰۰/۰< .(Pﻣﻴﺰﺍﻥ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﻨﻲ ﻭ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﻭ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺩﺭ ﺍﻓﺮﺍﺩ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﺩﺭ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ۳۶۲ ﻣﺮﺩ ۰۲ ﺗﺎ ۴۹ ﺳﺎﻟﻢ ﺑﺮﺭﺳﻲ ﺷﺪﻧﺪ ﮐﻪ ﺑﺮﺣﺴﺐ T-Scoreﻣﺤﻠﻲ ﺩﺭ ﺟﺪﻭﻝ ۵ ﻧﺸﺎﻥ ﺩﺍﺩﻩ ﺷﺪﻩﺍﺳﺖ. ﻣﻴﺎﻧﮕﻴﻦ ﺳﻦ ﺁﻧﻬﺎ ۳۶/۶۱±۶۴ ﺳﺎﻝ ﺑﻮﺩ. ﺑﺮﺍﻱ ﻣﻘﺎﻳﺴﻪ، ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﻨﻲ ﻭ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ ﺑﺎ ﻫﺮ ﺩﻭ ﺟﺪﻭﻝ ۱ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺗﻦﺳﻨﺠﻲ ﺍﻳﻦ ﺍﻓﺮﺍﺩ ﺭﺍ ﻧﺸﺎﻥ ﻣﻲﺩﻫﺪ. ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﻭ WHOﺩﺭ ﻧﻤﻮﺩﺍﺭﻫﺎﻳﻲ ﺭﺳﻢ ﺷﺪﻧﺪ. i - Dual Energy X-Ray Absorptiometry ii - Bone Mineral Content iii - Coefficient Variation
- 4. ﺩﻭﺭﻩﻱ ﺩﻭﺍﺯﺩﻫﻢ, ﺷﻤﺎﺭﻩﻱ ۴، ﺁﺑﺎﻥ ۹۸۳۱ ﻣﺠﻠﻪﻱ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ ﺍﻳﺮﺍﻥ ۶۹۳ ﺟﺪﻭﻝ ۲ ـ ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﻛﻢ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ) (PBMﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤـﺮ، ﮔـﺮﺩﻥ ﺍﺳـﺘﺨﻮﺍﻥ ﺭﺍﻥ ﻭ ﻛـﻞ ﺍﺳـﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺩﺭ ﻣـﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻳﻲ ﻛﻮﺍﺭ * Regression equation )PBM (95% CI ﺳﻦ ﺍﻳﺠﺎﺩ PBM ﻧﺎﺣﻴﻪ )ﮔﺮﻡ ﺑﺮ ﺳﺎﻧﺘﻲﻣﺘﺮ ﻣﺮﺑﻊ( )ﺳﺎﻝ( ۳y=۱/۲۴۴-۰/۰۰۸x-۰/۰۰۰۰۱۹x۲+۰/۰۰۰۰۰۰۴۵۹x )۴۰۳/۱ – ۹۰۸/۰( ۶۵۰/۱ )۴۲-۰۲( ۰۲ ﮔﺮﺩﻥ ﻓﻤﻮﺭ ۳y=۱/۰۹۳+۰/۰۰۰۰۸۸x+۰/۰۰۰۰۰۰۸۵۶x )۵۰۳/۱ – ۳۰۸/۰( ۴۵۰/۱ )۴۲-۰۲( ۰۲ ﻛﻞ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ۳y=۱/۲۲۷ +۰/۰۰۰۰۰۱۳۶x )۱۴۴/۱ – ۲۵۸/۰( ۶۴۱/۱ )۴۲-۰۲( ۰۲ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ * ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﺍﻳﻦ ﻓﺮﻣﻮﻝ ﺑﺎ ﻗﺮﺍﺭ ﺩﺍﺩﻥ ﺳﻦ )ﺑﺮ ﺣﺴﺐ ﺳﺎﻝ( ﺑﻪ ﺟﺎﻱ xﻣﻲﺗﻮﺍﻥ BMDﺭﺍ ﺑﺮﺣﺴﺐ ﮔﺮﻡ ﺑﺮ ﺳﺎﻧﺘﻲﻣﺘﺮ ﻣﺮﺑﻊ ﺑﻪ ﺩﺳﺖ ﺁﻭﺭﺩ. ﺟﺪﻭﻝ ۳ ـ ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﻛﻢ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﮔﺮﻭﻩ ﻣﺮﺟﻊ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ، ﮔﺮﺩﻥ ﺭﺍﻥ ﻭ ﻛﻞ ﺭﺍﻥ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻳﻲ ﻛﻮﺍﺭ ﺗﺮﺍﻛﻢ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻥ )ﮔﺮﻡ ﺑﺮ ﺳﺎﻧﺘﻲﻣﺘﺮ ﻣﺮﺑﻊ( ﺗﻌﺪﺍﺩ ﮔﺮﻭﻩ ﺳﻨﻲ )ﺳﺎﻝ( ﻧﺎﺣﻴﻪ ۳۱۱/۰±۵۹۰/۱ ۱۳ ۴۲-۰۲ ﮔﺮﺩﻥ ﺭﺍﻥ ۹۹۰/۰±۶۶۰/۱ ۱۳ ۴۲-۰۲ ﻛﻞ –ﺭﺍﻥ ۷۳۱/۰±۹۵۱/۱ ۱۳ ۴۲-۰۲ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ * ﺍﻋﺪﺍﺩ ﺑﻪ ﺻﻮﺭﺕ ﻣﻴﺎﻧﮕﻴﻦ±ﺍﻧﺤﺮﺍﻑ ﻣﻌﻴﺎﺭ ﺑﻴﺎﻥ ﺷﺪﻩﺍﻧﺪ. ﺟﺪﻭﻝ ۴ ـ ﻣﻴﺎﻧﮕﻴﻦ ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﻛﻢ ﺗـﻮﺩﻩﻱ ﺍﺳـﺘﺨﻮﺍﻧﻲ ) (PBMﺭﻭﺳـﺘﺎﻳﻴﺎﻥ ﮐـﻮﺍﺭ ﺩﺭ ﻣﻘﺎﻳـﺴﻪ ﺑـﺎ PBMﺍﺳـﺘﺎﻧﺪﺍﺭﺩ ﺩﺳـﺘﮕﺎﻩ )(WHO ﺑﻴﺸﺘﺮﻳﻦ ﺗﺮﺍﮐﻢ ﺍﺳﺘﺨﻮﺍﻥ )ﮔﺮﻡ ﺑﺮ ﺳﺎﻧﺘﻲﻣﺘﺮ ﻣﺮﺑﻊ( ﻣﻨﻄﻘﻪﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ † * ﻣﻘﺪﺍﺭ P ﺍﺧﺘﻼﻑ ﺍﺳﺘﺎﻧﺪﺍﺭﺩ ﺩﺳﺘﮕﺎﻩ ﺭﻭﺳﺘﺎﻳﻴﺎﻥ ﮐﻮﺍﺭ ‡ ۳۰/۰ ۷۴۰/۰+ ۲۱/۰±۸۴۰/۱ ۱۱/۰±۵۹۰/۱ ﮔﺮﺩﻥ ﺭﺍﻥ ۱۰۰/۰ ۵۳۰/۰+ ۴۱/۰±۱۳۰/۱ ۹۰/۰±۶۶۰/۱ ﮐﻞ-ﺭﺍﻥ ۱۰/۰ ۵۵۰/۰- ۲۱/۰±۴۱۲/۱ ۳۱/۰±۹۵۱/۱ ﻣﻬﺮﻩﻫﺎ * ﻣﻘﺪﺍﺭ ﺗﺮﺍﮐﻢ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﺭﻭﺳﺘﺎﻳﻴﺎﻥ ﮐﻮﺍﺭ ﻣﻨﻬﺎﻱ ﻣﻘﺪﺍﺭ ﺗﺮﺍﮐﻢ ﺍﺳﺘﺎﻧﺪﺍﺭﺩ، † ﻣﻴﺰﺍﻥ pﺍﺯ ﺁﺯﻣﻮﻥ ﺗﻲ ﺑﻪ ﺩﺳﺖ ﺁﻣﺪﻩ ﺍﺳﺖ. ﺟﺪﻭﻝ ۵ ـ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﻨﻲ ﻭ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﻭ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺩﺭ ﮔﺮﻭﻩﻫﺎﻱ ﺳﻨﻲ ﻣﺨﺘﻠﻒ ﺑﺮ ﺣﺴﺐ T-Scoreﻣﺤﻠﻲ )%( ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺍﺳﺘﺌﻮﭘﻨﻲ ﮔﺮﻭﻩ ﺳﻨﻲ ﮐﻞ ﺭﺍﻥ ﮔﺮﺩﻥ ﺭﺍﻥ ﮐﻤﺮ ﮐﻞ ﺭﺍﻥ ﮔﺮﺩﻥ ﺭﺍﻥ ﮐﻤﺮ ۴% ۲% ۰% ۴۱% ۲۲% ۶۱% ۹۲ – ۰۲ ۸/۱۱% ۸/۹% ۲% ۳/۳۳% ۳/۷۳% ۵/۳۲% ۹۳ – ۰۳ ۸/۵۱% ۱/۸۲% ۰% ۱/۲۴% ۱/۶۵% ۱۵% ۹۴ – ۰۴ ۶/۹% ۹/۶۲% ۸/۳% ۶/۹۵% ۷/۷۵% ۱۶% ۹۵ – ۰۵ ۱/۲۳% ۸/۵۵% ۲/۳۱% ۹/۰۵% ۵/۸۳% ۸/۵۳% ۰۶ ≥ ۸/۴۱% ۸/۴۲% ۸/۳% ۳/۰۴% ۷/۲۴% ۸۳% ﮐﻞ
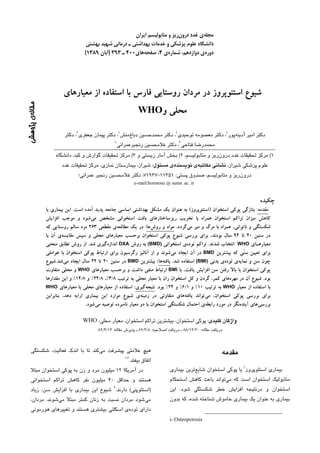
- 5. ۷۹۳ ﺍﻭﺳﺘﺌﻮﭘﺮﻭﺯ ﺩﺭ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻫﺎﻱ ﻓﺎﺭﺱ ﺩﻛﺘﺮ ﺍﻣﻴﺮ ﺁﺩﻳﻨﻪﭘﻮﺭ ﻭ ﻫﻤﻜﺎﺭﺍﻥ 06 WHO ﻫﻤﺎﻫﻨﮓ ﺑﺎ ﺳﻦ ﻭ BMIﺩﺭ ﺍﻳﻦ، ﻣﺸﺎﺑﻪ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺳﺎﻳﺮ ۱۱،۹،۸،۷،۱ 05 ﻫﻢﭼﻨﻴﻦ، ﻣﻄﺎﻟﻌﻪﻫﺎ ﺩﺭ ﺍﻳﺮﺍﻥ ﻭ ﺩﻳﮕﺮ ﮐﺸﻮﺭﻫﺎ ﺑﻮﺩ. ﺑﺮﺍﺳﺎﺱ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺍﻳﻦ ﺑﺮﺭﺳﻲ، ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻳﻲ ﮐﻮﺍﺭ ﺩﺭ 04 ﺩﺭﺻﺪ ﺳﻦ ۰۲ ﺗﺎ ۴۲ ﺳﺎﻝ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ، ﮔﺮﺩﻥ ﺭﺍﻥ ﻭ ﺩﺭ ﻛﻞ ﺭﺍﻥ ﺑﻪ ﺑﻴﺸﺘﺮﻳﻦ ﺗﻮﺩﻩﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﻲﺭﺳﻨﺪ. ﺳﻦ ﺭﺳﻴﺪﻥ ﺑﻪ PBM 03 ﺩﺭ ﻣﺮﺩﺍﻥ ﮐﻮﺍﺭﻱ ﮐﻤﺘﺮ ﻳﺎ ﻣﺴﺎﻭﻱ ﺑﺎ ﺳﻨﻲ ﺍﺳﺖ ﮐﻪ ﺩﺭ ﺳﺎﻳﺮ 02 ﻣﻄﺎﻟﻌﻪﻫﺎ ﺫﮐﺮ ﺷﺪﻩ ﺍﺳﺖ. ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻳﻲ ﻣﻌﻤﻮﻻ ﺍﺯ ﺳﻨﻴﻦ ﹰ 01 ﭘﺎﻳﻴﻦﺗﺮ ﺑﻪ ﮐﺎﺭ ﺩﺭ ﻣﺰﺭﻋﻪ ﻭ ﻓﻌﺎﻟﻴﺖ ﻣﺸﻐﻮﻝ ﻣﻲﺷﻮﻧﺪ ﻭ ﺍﺯ ﺁﻥ ﺟﺎ ﻛﻪ ﺷﺮﻭﻉ ﻓﻌﺎﻟﻴﺖ ﺩﺭ ﺳﻦ ﭘﺎﻳﻴﻦ ﻭ ﺷﺪﺕ ﺁﻥ ﺑﺎ ﺯﻣﺎﻥ 0 ۴۱،۳۱ ﺷﺎﻳﺪ ﺑﺘﻮﺍﻥ ﺯﻣﺎﻥ ﺯﻭﺩﺭﺱ ﺭﺳﻴﺪﻥ ﺑﻪ PBMﺍﺭﺗﺒﺎﻁ ﺩﺍﺭﺩ، ﻣﻬﺮﻩﻫﺎ ﮔﺮﺩﻥ ﺭﺍﻥ ﻛﻞ ﺭﺍﻥ PBMﺭﺍ ﺩﺭ ﻣﺮﺩﺍﻥ ﮐﻮﺍﺭﻱ ﻧﺴﺒﺖ ﺑﻪ ﺳﺎﻳﺮ ﻣﻄﺎﻟﻌﻪﻫﺎ ﺑﻪ ﺍﻳﻦ ﻣﻨﻄﻘﻪﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﻮﺿﻮﻉ ﻧﺴﺒﺖ ﺩﺍﺩ. ﻧﻤﻮﺩﺍﺭ ۱ـ ﻣﻘﺎﻳﺴﻪ ﺷﻴﻮﻉ ﺍﺳـﺘﺌﻮﭘﻨﻲ )ﺩﺭﺻـﺪ( ﺑـﺮ ﺍﺳـﺎﺱ ﺩﺭ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﻧﺸﺎﻥ ﺩﺍﺩﻩ ﺷﺪ ﻛﻪ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﻌﻴﺎﺭﻫـــﺎﻱ WHOﻭ ﻣﻌﻴﺎﺭﻫـــﺎﻱ ﻣﺤﻠـــﻲ ﺩﺭ ﻣـــﺮﺩﺍﻥ ـ ـ ـ ـ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻳﻲ ﺑﺮﺍﺳﺎﺱ ﻣﻌﻴﺎﺭ ،WHO ﺭﻭﺳﺘﺎﻫﺎﻳﻲ ﻛﻮﺍﺭ ۴۲% ﺍﺳﺖ ﺩﺭﺣﺎﻟﻲﻛﻪ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻘﻴﺎﺱ ﻣﺤﻠﻲ ﺍﻳﻦ ﻣﻴﺰﺍﻥ ﺑﻪ ۸/۳% ﺭﺳﻴﺪ. ﻫﻢﭼﻨﻴﻦ، ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﮔﺮﺩﻥ ﺭﺍﻥ ﻭ 03 WHO ﻛﻞ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭ WHOﺑﻪ ﺗﺮﺗﻴﺐ ۰۱% 52 ﻭ ۱/۶% ﺑﻮﺩ ﮐﻪ ﺑﺮ ﺍﺳﺎﺱ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﺍﻳﻦ ﻣﻘﺪﺍﺭﻫﺎ ﺍﻓﺰﺍﻳﺶ ﻳﺎﻓﺖ ﻭ ﺩﺭ ﮔﺮﺩﻥ ﺭﺍﻥ ﺑﻪ ۸/۴۲% ﻭ ﺩﺭ ﻛﻞ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺑﻪ 02 ۸/۴۱% ﺭﺳﻴﺪ. ﺩﺭ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ ﻣﺘﻌﺪﺩﻱ ﮐﻪ ﺍﺯ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﺑﺮﺍﻱ ﺩﺭﺻﺪ 51 ﺑﺮﺭﺳﻲ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺍﺳﺘﻔﺎﺩﻩ ﺷﺪﻩ ﺍﺳﺖ، ﺍﻳﻦ ﺍﺧﺘﻼﻑﻫﺎ ﮐﻢ ﻭ ﺑﻴﺶ ﺩﺭ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﺩﻭ ﻣﻌﻴﺎﺭ ﻭﺟﻮﺩ 01 ﺩﺍﺷﺘﻪﺍﺳﺖ: ﺑﻪ ﻋﻨﻮﺍﻥ ﻣﺜﺎﻝ ﺩﺭ ﻣﻄﺎﻟﻌﻪﻱ ﺩﻛﺘﺮ ﻋﻤﺮﺍﻧﻲ ﺩﺭ 5 ﺷﻴﺮﺍﺯ، ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭ WHOﺩﺭ ﮔﺮﺩﻥ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ، ۳% ﺑﻪ ﺩﺳﺖ ﺁﻣﺪ ﺩﺭﺣﺎﻟﻲﻛﻪ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ 0 ۷ ﺍﺯ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ، ﺑﻪ ۱/۲% ﺭﺳﻴﺪ. ﻫﻢﭼﻨﻴﻦ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﻣﻬﺮﻩﻫﺎ ﮔﺮﺩﻥ ﺭﺍﻥ ﻛﻞ ﺭﺍﻥ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﻣﺮﺩﺍﻥ ﺷﻴﺮﺍﺯﻱ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻨﻄﻘﻪﻱ ﺍﺳﺘﺨﻮﺍﻧﻲ ﻣﻌﻴﺎﺭ ﺭﻓﺮﺍﻧﺲ WHOﻭ ﻣﺤﻠﻲ ﺑﻪ ﺗﺮﺗﻴﺐ ۴/۶۱% ﻭ ۴/۳۱% ﻧﻤﻮﺩﺍﺭ ۲ ـ ﻣﻘﺎﻳﺴﻪﻱ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ )ﺩﺭﺻﺪ( ﺑﺮ ﺍﺳﺎﺱ ۷ ﺑﻮﺩ. ﺩﺭ ﻣﻄﺎﻟﻌﻪﻱ ﭼﻨﺪ ﻣﺮﮐﺰﻱ ﺍﻳﺮﺍﻥ ) (IMOSﻧﺸﺎﻥ ﺩﺍﺩﻩ ﺷﺪ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﻭ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﺩﺭ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻫﺎﻱ ﻛﻮﺍﺭ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺩﺭ ﻣﺮﺩﺍﻥ ۰۵ ﺳﺎﻟﻪ ﻳﺎ ﺑﺎﻻﺗﺮ ﻃﺒﻖ ﻣﻌﻴﺎﺭﻫﺎﻱ ﺁﻣﺮﻳﮑﺎ ﻭ IMOSﺑﻪ ﺗﺮﺗﻴﺐ،۳ ﺩﺭﺻﺪ ﻭ ۷/۲% ﻭ ﺑﺤﺚ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﮐﻤﺮ ﺑﻪ ﺗﺮﺗﻴﺐ ۲/۴۱% ﻭ ۵/۳% ﺑﻮﺩ ﻛﻪ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﺩﺭ ﺣﺎﻝ ﺣﺎﺿﺮ ﺍﻭﻟﻴﻦ ﺑﺮﺭﺳﻲ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﻧﺸﺎﻥﺩﻫﻨﺪﻩﻱ ﺗﻔﺎﻭﺕ ﺁﺷﮑﺎﺭ ﻣﻌﻴﺎﺭ WHOﺩﺳﺘﮕﺎﻩ ﺑﺎ ﻣﻌﻴﺎﺭ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺮﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﺩﺭ ﮔﺮﻭﻫﻲ ﺍﺯ ﻣﺮﺩﺍﻥ ﺳﺎﻟﻢ ﻣﺤﻠﻲ ﺍﺳﺖ.۸ ﺩﺭ ﻣﻄﺎﻟﻌﻪﺍﻱ ﻛﻪ ﺩﺭ ﻋﺮﺑﺴﺘﺎﻥ ﺳﻌﻮﺩﻱ ﺍﻧﺠﺎﻡ ﺭﻭﺳﺘﺎﻳﻲ ﮐﻮﺍﺭ ﻓﺎﺭﺱ ﻭ ﻣﻘﺎﻳﺴﻪﻱ ﺁﻥ ﺑﺎ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺷﺪ، ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﮐﻤﺮﻱ ﺑﺎ ﻣﻌﻴﺎﺭ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺮ ﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﺍﺳﺖ. ﺁﻣﺮﻳﻜﺎﻳﻲ ﮐﻤﺘﺮ ﺍﺯ ﺷﻴﻮﻉ ﺁﻥ ﺑﺮﺍﺳﺎﺱ ﻣﻌﻴﺎﺭ ﺳﻌﻮﺩﻱ ﺑﻮﺩ ﺑﺮﺍﺳﺎﺱ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ )۳/۸۳% ﺩﺭ ﻣﻘﺎﺑﻞ ۹/۹۴%(، ﺩﺭﺣﺎﻟﻲﮐﻪ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺍﻓﺰﺍﻳﺶ ﺳﻦ ﺑﻴﺸﺘﺮ ﻭ ﺑﺎ ﺍﻓﺰﺍﻳﺶ ﻭﺯﻥ ﮐﻤﺘﺮ ﻣﻲﺷﻮﺩ. ﺗﻐﻴﻴﺮﺍﺕ ﺩﺭ ﮐﻞ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﻃﺒﻖ ﻣﻌﻴﺎﺭﻫﺎﻱ ﺳﻌﻮﺩﻱ ﮐﻤﺘﺮ ﺍﺯ ﺷﻴﻮﻉ
- 6. ﺩﻭﺭﻩﻱ ﺩﻭﺍﺯﺩﻫﻢ, ﺷﻤﺎﺭﻩﻱ ۴، ﺁﺑﺎﻥ ۹۸۳۱ ﻣﺠﻠﻪﻱ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ ﺍﻳﺮﺍﻥ ۸۹۳ ﮐﻪ ﺩﺭ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺗﺄﺛﻴﺮﮔﺬﺍﺭ ﻫﺴﺘﻨﺪ ﺩﺭ ﺭﻭﺳﺘﺎﻳﻲﻫﺎ ﺑﺎﻻﺗﺮ ﺑﺮ ﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﺑﻪ ﺩﺳﺖ ﺁﻣﺪ. ﻳﺎﻓﺘﻪﻫﺎ ﺩﺭ ﺯﻧﺎﻥ ﺑﻮﺩﻩ ﻭ ﺣﺘﻲ ﻧﺴﺒﺖ ﺑﻪ ﺷﻬﺮﻧﺸﻴﻨﺎﻥ ﺁﻥ ﻣﻨﺎﻃﻖ ﺷﺎﻳﻊﺗﺮ ﺍﺳﺖ. ﺳﻌﻮﺩﻱ ﮐﻤﻲ ﻣﺘﻔﺎﻭﺕ ﺑﻮﺩ ﺑﻪ ﺍﻳﻦ ﺗﺮﺗﻴﺐ ﻛﻪ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺑﻨﺎﺑﺮﺍﻳﻦ، ﺍﺣﺘﻤﺎﻝ ﺍﻳﻦ ﮐﻪ ﻣﺼﺮﻑ ﻣﻮﺍﺩ ﺩﺍﺭﺍﻱ ﮐﻠﺴﻴﻢ ﺩﺭ ﺍﺳﺘﺨﻮﺍﻥ ﻫﻢ ﺩﺭ ﺭﺍﻥ ﻭ ﻫﻢ ﺩﺭ ﻣﻬﺮﻩﻫﺎﻱ ﮐﻤﺮﻱ ﺑﺮﺍﺳﺎﺱ ﺭﻭﺳﺘﺎﻳﻲﻫﺎ ﮐﻤﺘﺮ ﺑﺎﺷﺪ ﻳﺎ ﻋﺎﺩﺍﺕﻫﺎﻳﻲ ﻣﺎﻧﻨﺪ ﺳﻴﮕﺎﺭ ﮐﺸﻴﺪﻥ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﮐﻤﺘﺮ ﺍﺯ ﻣﻌﻴﺎﺭ WHOﺑﻮﺩ.۹ ﺩﺭ ﻣﻄﺎﻟﻌﻪﺍﻱ ﮐﻪ ﺑﻴﺸﺘﺮ ﺑﺎﺷﺪ، ﻭﺟﻮﺩ ﺩﺍﺭﺩ. ﺑﺨﺼﻮﺹ ﻛﻪ ﺩﺭ ﻣﻄﺎﻟﻌﻪﻱ ﮔﻮﻭ ﻭ ﺩﺭ ﭼﻴﻦ ﺗﻮﺳﻂ ﻭﻭ ﻭ ﻫﻤﮑﺎﺭﺍﻥ ﺍﻧﺠﺎﻡ ﮔﺮﻓﺖ، ﺩﻳﺪﻩ ﺷﺪ ﻛﻪ ﻫﻤﮑﺎﺭﺍﻥ، ﻣﺼﺮﻑ ﮐﻢ ﻣﻮﺍﺩ ﺩﺍﺭﺍﻱ ﮐﻠﺴﻴﻢ ﻭ ﺷﻴﻮﻉ ﺑﺎﻻﺗﺮ ﺑﺮﺍﺳﺎﺱ ﻣﻌﻴﺎﺭﻫﺎﻱ ﭼﻴﻨﻲ ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ ﺩﺭ ﮔﺮﺩﻥ ﻋﺎﺩﺕﻫﺎﻳﻲ ﻣﺎﻧﻨﺪ ﺳﻴﮕﺎﺭ ﮐﺸﻴﺪﻥ ﺩﺭ ﺭﻭﺳﺘﺎﻳﻲﻫﺎ ﺍﺯ ﺩﻻﻳﻞ ﮐﻤﺘﺮ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ۹۰۱% ﺑﻴﺸﺘﺮ ﺍﺯ ﺷﻴﻮﻉ ﺁﻥ ﺑﺮ ﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ ﺑﻮﺩﻥ BMDﻭ ﺷﻴﻮﻉ ﺑﺎﻻﻱ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺁﻧﻬﺎ ﺫﻛﺮ WHOﺑﻮﺩ. ﻫﻢﭼﻨﻴﻦ، ﺷﻴﻮﻉ ﺍﺳﺘﺌﻮﭘﺮﻭﺯ ﻣﻬﺮﻩﻫﺎﻱ ﻛﻤﺮ ﺑﺮﻃﺒﻖ ۱۲ ﺷﺪﻩﺍﺳﺖ. ﺟﺜﻪﻱ ﻣﺮﺩﺍﻥ ﻭ BMIﺍﺯ ﻋﻮﺍﻣﻞ ﻣﺆﺛﺮ ﺑﺮ BMDﻭ ﻣﻌﻴﺎﺭﻫﺎﻱ ﭼﻴﻨﻲ ۱۳% ﺑﻴﺸﺘﺮ ﺍﺯ ﺷﻴﻮﻉ ﺁﻥ ﺑﺎ ﻣﻌﻴﺎﺭ WHO ۰۱ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﻲﺑﺎﺷﻨﺪ ﺩﺭ ﻣﻄﺎﻟﻌﻪﺍﻱ ﺩﺭ ﻧﺮﻭﮊ ﺑﻌﺪ ﺍﺯ ﺗﻌﺪﻳﻞ ﺑﻮﺩ. ﮐﺮﺩﻥ ﻋﻮﺍﻣﻞ ﺗﻐﺬﻳﻪﺍﻱ ﻭ ﺭﻓﺘﺎﺭﻱ، BMIﻳﮑﻲ ﺍﺯ ﻋﻮﺍﻣﻞ ﺍﺯ ﻋﻠﻞ ﻣﻬﻢ ﺗﻔﺎﻭﺕ ﺩﺭ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺗﺄﺛﻴﺮﮔﺬﺍﺭ ﺑﺮ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺭﻭﺳﺘﺎﻫﺎﻱ ﻣﻮﺭﺩ ﺍﺯ ﺩﻭ ﻣﻌﻴﺎﺭ، ﻋﻮﺍﻣﻠﻲ ﻫﺴﺘﻨﺪ ﻛﻪ ﺩﺭ ﻣﺤﺎﺳﺒﻪﻱ T-scoreﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﮔﺰﺍﺭﺵ ﺷﺪ.۳۱ ﺑﻴﻤﺎﺭﺍﻥ ﻣﻄﺎﻟﻌﻪﻱ ﻣﺎ ﻧﻴﺰ ﺑﻴﺸﺘﺮ ﺩﺍﺭﺍﻱ ﺍﺳﺘﻔﺎﺩﻩ ﻗﺮﺍﺭ ﻣﻲﮔﻴﺮﻧﺪ. PBMﻭ ﺍﻧﺤﺮﺍﻑ ﻣﻌﻴﺎﺭ، ﺩﻭ ﻋﺎﻣﻞ BMIﻃﺒﻴﻌﻲ ﻳﺎ ﭘﺎﻳﻴﻦ ﺑﻮﺩﻧﺪ ﮐﻪ ﺷﺎﻳﺪ ﺍﺯ ﻋﻠﺖﻫﺎﻱ ﻣﺆﺛﺮ ﺑﺮ ﺑﺴﻴﺎﺭ ﻣﻬﻢ ﺩﺭ ﺗﻌﻴﻴﻦ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﻫﺴﺘﻨﺪ ﮐﻪ ﺑﺎﻋﺚ ﺑﻪ ﺩﺳﺖ ﺗﺮﺍﮐﻢ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺟﻤﻌﻴﺖ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﺑﺎﺷﺪ. ﺑﺎ ﺑﺮﺭﺳﻲ ﺁﻣﺪﻥ ﻧﺘﺎﻳﺞ ﻣﺘﻔﺎﻭﺕ ﺩﺭﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﻲﺷﻮﻧﺪ. ﺍﺯ ﮊﻧﺘﻴﮏ ﻭ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ ﺍﭘﻴﺪﻣﻴﻮﻟﻮﮊﻳﮏ ﻭﺳﻴﻊ ﻭ ﮐﺎﻣﻞ ﺩﺭ ﻣﺮﺩﺍﻥ ﺁﻥﺟﺎ ﻛﻪ PBMﺍﺯ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺳﻨﺠﺶ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﮔﺮﻭﻩ ﺭﻭﺳﺘﺎﻳﻲ ﮐﻮﺍﺭ ﺷﺎﻳﺪ ﺑﺘﻮﺍﻥ ﭘﺎﺳﺨﻲ ﺑﺮﺍﻱ ﺗﻔﺎﻭﺕ ﺩﺭ ﺷﻴﻮﻉ ﻣﺮﺟﻊ ﺑﻪ ﺩﺳﺖ ﻣﻲﺁﻳﺪ، ﺷﺎﻳﺪ ﺑﺘﻮﺍﻥ ﺍﻳﻦ ﺗﻔﺎﻭﺕﻫﺎ ﺭﺍ ﺩﺭ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺮﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ WHOﻭ ﻣﺤﻠﻲ ﭘﻴﺪﺍ ﮐﺮﺩ ﻭ ﺧﺼﻮﺻﻴﺎﺕ ﮔﺮﻭﻩ ﻣﺮﺟﻊ ﺟﺴﺘﺠﻮ ﮐﺮﺩ ﺑﻪ ﻋﻨﻮﺍﻥ ﻣﺜﺎﻝ ﮊﻧﺘﻴﮏ، ﻫﻢﭼﻨﻴﻦ، ﺑﺎﻻ ﺑﻮﺩﻥ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺭﻭﺳﺘﺎﻫﺎﻱ ﮐﻮﺍﺭ ﻗﻮﻣﻴﺖ، ﻋﺎﺩﺕﻫﺎﻱ ﻏﺬﺍﻳﻲ- ﺭﻓﺘﺎﺭﻱ )ﻣﺎﻧﻨﺪ ﺳﻴﮕﺎﺭ ﮐﺸﻴﺪﻥ(، ﺭﺍ ﺗﻮﺟﻴﻪ ﻧﻤﻮﺩ. ﻭﻳﮋﮔﻲﻫﺎﻱ ﻓﻴﺰﻳﮑﻲ )ﺟﺜﻪ ﻭ BMIﻭ ﻭﺿﻌﻴﺖ ﺍﻗﺘﺼﺎﺩﻱ- ﻣﻘﺪﺍﺭ PBMﺭﻭﺳﺘﺎﻳﻲﻫﺎ ﺩﺭ ﺩﻭ ﻧﺎﺣﻴﻪﻱ ﮔﺮﺩﻥ ﺭﺍﻥ ﻭ ﮐﻞ ﺍﺟﺘﻤﺎﻋﻲ( ﻣﺘﻔﺎﻭﺕ ﺩﺭ ﮔﺮﻭﻩ ﻣﺮﺟﻊ ﮐﻪ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺁﻧﻬﺎ ﺍﺳﺘﺨﻮﺍﻥ ﺭﺍﻥ ﺩﺭ ﻣﻘﺎﻳﺴﻪ ﺑﺎ ﺍﺳﺘﺎﻧﺪﺍﺭﺩ ﺩﺳﺘﮕﺎﻩ ﺑﺎﻻﺗﺮ ﺑﻮﺩ. ﺑﺎ ﻣﻘﺎﻳﺴﻪ ﻣﻲﺷﻮﺩ ﻭ ﻫﻢﭼﻨﻴﻦ ﺩﺭ ﮐﻞ ﺟﻤﻌﻴﺖ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﺍﺯ ﻭﺟﻮﺩ ﺑﺎﻻ ﺑﻮﺩﻥ ﺍﻳﻦ ﻣﻘﺪﺍﺭﻫﺎ، ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺍﻳﻦ ﻧﻘﺎﻁ ﺟﻤﻠﻪ ﺍﻳﻦ ﺧﺼﻮﺻﻴﺎﺕ ﻫﺴﺘﻨﺪ. ﺩﺭ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﮔﺮﻭﻩ ﻣﺮﺟﻊ ﮐﻪ ﺍﺳﺘﺨﻮﺍﻧﻲ ﺑﻴﺸﺘﺮ ﺑﻮﺩ. ﺑﻪ ﻧﻈﺮ ﻣﻲﺭﺳﺪ ﻛﻪ ﻣﺮﺩﺍﻥ ﮐﻮﺍﺭﻱ PBMﺁﻧﻬﺎ ﺑﻪ ﻋﻨﻮﺍﻥ ﻣﻌﻴﺎﺭ ﺗﻌﻴﻴﻦ T-Scoreﺍﺳﺘﻔﺎﺩﻩ ﺷﺪ، ﺩﭼﺎﺭ ﺍﻓﺖ ﺳﺮﻳﻊ ﺗﺮﺍﮐﻢ ﺍﺳﺘﺨﻮﺍﻥ ﺑﻪ ﺧﺼﻮﺹ ﺩﺭ ﮔﺮﺩﻥ ﺭﺍﻥ ﻣﺮﺩﺍﻥ ۰۲ ﺗﺎ ۴۲ ﺳﺎﻟﻪ ﺑﻮﺩﻧﺪ. ﺩﺭ ﺳﺎﻳﺮ ﻣﻄﺎﻟﻌﻪﻫﺎﻳﻲ ﮐﻪ ﺍﺯ ﺑﺎﺷﻨﺪ. ﺑﺮﺭﺳﻲ ﻛﺎﻣﻞ ﺍﺯ ﻧﻈﺮ ﺍﺛﺒﺎﺕ ﮐﺎﻫﺶ ﺗﺮﺍﮐﻢ ﻭ ﻋﻠﺖﻫﺎﻱ ﺁﻥ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﺍﺳﺘﻔﺎﺩﻩ ﮐﺮﺩﻩﺍﻧﺪ، ﻃﻴﻒ ﺳﻨﻲ ﻣﺨﺘﻠﻔﻲ ﺍﺳﺘﻔﺎﺩﻩ ﺷﺎﻳﺪ ﭘﺎﺳﺨﻲ ﺑﺮﺍﻱ ﺳﺆﺍﻻﺕ ﻣﺎ ﺑﺎﺷﺪ. ۰۲ ﺗﺎ ۵۳ ﺳﺎﻝ،۹ ۹۱ ﺗﺎ ۵۲ ۰۱،۷ ﺷﺪﻩﺍﺳﺖ: ﺳﻦ ۰۲ ﺗﺎ ۴۲ ﺳﺎﻝ ﺍﻣﻴﺪ ﺑﻪ ﺯﻧﺪﮔﻲ ﻭ ﺩﺭ ﻧﺘﻴﺠﻪ ﺳﻦ ﺟﺎﻣﻌﻪﻱ ﺭﻭﺳﺘﺎﻳﻲ ﺭﻭ ﺑﻪ ﺳﺎﻝ.۶۱،۵۱ ﮔﺮﻭﻩ ﻣﺮﺟﻊ WHOﻧﻴﺰ ﺷﺎﻣﻞ ﺳﻨﻴﻦ ۰۲ ﺗﺎ ۴۴ ﺳﺎﻝ ﺍﻓﺰﺍﻳﺶ ﺍﺳﺖ، ﻫﻢﭼﻨﻴﻦ، ﺳﺒﮏ ﺯﻧﺪﮔﻲ ﺷﻬﺮﻱ ﻧﻴﺰ ﺭﻭ ﺑﻪ ﻣﻲﺑﺎﺷﺪ ﻛﻪ ﻃﻴﻒ ﺳﻨﻲ ﻭﺳﻴﻊﺗﺮﻱ ﺩﺍﺭﺩ ﻭ ﺗﻌﺪﺍﺩ ﺑﻴﺸﺘﺮﻱ ﺭﺍ ﮔﺴﺘﺮﺵ ﻣﻲﺑﺎﺷﺪ ﻛﻪ ﺍﻳﻦ ﻋﻠﻞ ﺑﻪ ﻋﻮﺍﻣﻞ ﺑﻨﻴﺎﺩﻱ ﻣﺎﻧﻨﺪ ﮐﻤﻲ ﺷﺎﻣﻞ ﻣﻲﺷﻮﺩ. ﺑﻨﺎﺑﺮﺍﻳﻦ ﺍﻳﻦ ﺍﺧﺘﻼﻑ ﺩﺭ ﻃﻴﻒ ﺳﻨﻲ ﻭ ﺗﻌﺪﺍﺩ ۰۱،۱ ﺁﮔﺎﻫﻲ ﺭﻭﺳﺘﺎﻳﻲﻫﺎ ﺍﺯ ﻋﻮﺍﻣﻞ ﺧﻄﺮﺳﺎﺯ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺍﺿﺎﻓﻪ ﺍﻓﺮﺍﺩ ﮔﺮﻭﻩ ﺷﺎﻫﺪ ﻣﻲﺗﻮﺍﻧﺪ ﺑﺮ ﻳﺎﻓﺘﻪﻫﺎ ﺗﺄﺛﻴﺮ ﺑﮕﺬﺍﺭﺩ. ﻣﻲﺷﻮﺩ. ﭘﺲ ﺷﺎﻳﺪ ﺩﺭ ﺁﻳﻨﺪﻩ ﺷﺎﻫﺪ ﺷﻴﻮﻉ ﺑﻴﺸﺘﺮ ﭘﻮﮐﻲ ﻋﻮﺍﻣﻞ ﮊﻧﺘﻴﮑﻲ ﻣﺘﻌﺪﺩ ﻭ ﻗﻮﻣﻴﺖ ﻣﻲﺗﻮﺍﻧﻨﺪ ﺍﺯ ﻋﻠﻞ ﺗﻔﺎﻭﺕ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ﺍﻳﻦ ﺟﻮﺍﻣﻊ ﺑﺎﺷﻴﻢ. ﺩﺭﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺮ ﺣﺴﺐ ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﺑﺎﺷﻨﺪ. ﺩﺭ ﻧﻈﺮ ﺑﻪ ﺍﻳﻦ ﮐﻪ ﺭﺍﻫﻨﻤﺎﻱ ﺟﺪﻳﺪ ﺭﻭﺵ ﺑﺮﺧﻮﺭﺩ ﺑﺎ ﭘﻮﮐﻲ ﺑﺮﺭﺳﻲﻫﺎﻱ ﮊﻧﺘﻴﮑﻲ ﻭﺟﻮﺩ ﻣﺤﻞﻫﺎﻱ ﮊﻧﻲ ﻣﺎﻧﻨﺪ 5،LPR ﺍﺳﺘﺨﻮﺍﻥ، ﻣﺒﺘﻨﻲ ﺑﺮ ﺳﻬﻴﻢ ﺑﻮﺩﻥ ﻋﻮﺍﻣﻞ ﺧﻄﺮﺳﺎﺯ ﺑﺎﻟﻴﻨﻲ ﻣﺎﻧﻨﺪ 1 ESRﻭ OPGﺭﺍ ﺍﺯ ﻋﻮﺍﻣﻞ ﻣﺆﺛﺮ ﺑﺮ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺩﺭ ۰۲-۷۱ ﺳﻦ، ﺟﻨﺲ، ﻗﺪ، ﻭﺯﻥ، ﺳﺎﺑﻘﻪﻱ ﺷﻜﺴﺘﮕﻲ ﺩﺭ ﻓﺮﺩ ﻭ ﻭﺍﻟﺪﻳﻦ ﻫﻢﭼﻨﻴﻦ ﻭﺿﻌﻴﺖ ﻗﻮﻣﻴﺖﻫﺎﻱ ﻣﺨﺘﻠﻒ ﺫﮐﺮ ﮐﺮﺩﻩﺍﻧﺪ ﺳﻴﮕﺎﺭ ﻛﺸﻴﺪﻥ، ﻣﺼﺮﻑ ﺍﺳﺘﺮﻭﺋﻴﺪﻫﺎ، ﺑﻴﻤﺎﺭﻱ ﺭﻭﻣﺎﺗﻴﺴﻢ ﺗﻐﺬﻳﻪﺍﻱ ﻭ ﺧﺼﻴﺼﻪﻫﺎﻱ ﺭﻓﺘﺎﺭﻱ ﻣﺎﻧﻨﺪ ﺳﻴﮕﺎﺭ ﮐﺸﻴﺪﻥ ۱۲ ﻣﻔﺼﻠﻲ، ﻣﺼﺮﻑ ﺍﻟﻜﻞ، ﻣﻴﺰﺍﻥ BMDﻭ ﻧﻮﻉ ﺩﺳﺘﮕﺎﻩ ﺳﻨﺠﺶ ﺩﺭ ﭼﻨﺪ ﻣﻲﺗﻮﺍﻧﺪ ﺑﺮ ﺷﻴﻮﻉ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﻣﺆﺛﺮ ﺑﺎﺷﺪ. ۳۲ ﺗﺮﺍﻛﻢ ﺍﺳﺘﺨﻮﺍﻥ ﻣﻲﺑﺎﺷﺪ ) ، (FRAX Toolﺑﻨﺎﺑﺮﺍﻳﻦ ﺩﺭ ﻳﮏ ﻣﻄﺎﻟﻌﻪ ﺩﻳﺪﻩ ﺷﺪﻩ ﺍﺳﺖ ﮐﻪ ﻋﺎﺩﺕﻫﺎﻱ ﻏﺬﺍﻳﻲ ﻭ ﺭﻓﺘﺎﺭﻱ ﺧﺎﺻﻲ
- 7. ۳۹۹ ﺍﻭﺳﺘﺌﻮﭘﺮﻭﺯ ﺩﺭ ﻣﺮﺩﺍﻥ ﺭﻭﺳﺘﺎﻫﺎﻱ ﻓﺎﺭﺱ ﺩﻛﺘﺮ ﺍﻣﻴﺮ ﺁﺩﻳﻨﻪﭘﻮﺭ ﻭ ﻫﻤﻜﺎﺭﺍﻥ ﺭﺍ ﺩﺭ ﻣﺮﺩﺍﻥT-score ﻭBMD ﺟﻤﻊﺑﻨﺪﻱ ﺍﻃﻼﻋﺎﺕ، ﻣﻨﺒﻊ ﺑﺮﺧﻮﺭﺩ ﻣﻨﺎﺳﺐ ﺑﺎ ﭘﻮﮐﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎﻳﺪ ﺍﺯ ﺗﻤﺎﻡ ﻋﻠﺖﻫﺎ ﻭ ﺭﻭﺳﺘﺎﻳﻲ ﺍﻳﺮﺍﻧﻲ ﻣﻲﺗﻮﺍﻥ ﺗﻌﻴﻴﻦ ﻛﺮﺩ ﻭ ﺍﺯ ﺧﻄﺮﻫﺎﻱ ﻧﺎﺷﻲ ﺍﺯ ، ﺍﺳﺘﻔﺎﺩﻩT-Score ﻋﻮﺍﻣﻞ ﻣﺆﺛﺮ ﺩﺭ ﻭﻗﻮﻉ ﺷﮑﺴﺘﮕﻲ، ﻧﻪ ﻓﻘﻂ .ﺍﻳﻦ ﺑﻴﻤﺎﺭﻱ ﺟﻠﻮﮔﻴﺮﻱ ﻧﻤﻮﺩ ﮐﺮﺩ. ﻫﻢﭼﻨﻴﻦ، ﺑﻪ ﻋﻠﺖ ﺍﻳﻦ ﮐﻪ ﺑﺎ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ﻣﻌﻴﺎﺭ ﻣﺤﻠﻲ ﻳﺎ ﺩﺭ ﻣﺠﻤﻮﻉ ﺑﺮ ﺍﺳﺎﺱ ﻳﺎﻓﺘﻪﻫﺎﻱ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﺍﺳﺘﻔﺎﺩﻩ ﺍﺯ ، ﻣﻤﻜﻦ ﺍﺳﺖ ﺗﺸﺨﻴﺺ، ﺑﻴﺸﺘﺮ ﻳﺎ ﮐﻤﺘﺮ ﺍﺯ ﺣﺪ ﻭﺍﻗﻌﻲWHO ﺑﺮﺍﻱ ﺑﺮﺭﺳﻲ ﭘﻮﮐﻲWHO ﻣﻌﻴﺎﺭﻫﺎﻱ ﻣﺤﻠﻲ ﻳﺎ ﻣﻌﻴﺎﺭﻫﺎﻱ ،ﮔﺰﺍﺭﺵ ﺷﻮﺩ، ﻭ ﻫﺰﻳﻨﻪﻫﺎﻱ ﺑﺨﺶ ﺩﺭﻣﺎﻥ ﺳﻨﮕﻴﻦﺗﺮ ﮔﺮﺩﺩ ﺍﺳﺘﺨﻮﺍﻥ، ﻣﻤﻜﻦ ﺍﺳﺖ ﻧﺘﺎﻳﺞ ﻣﺘﻔﺎﻭﺗﻲ ﺩﺭ ﺷﻴﻮﻉ ﺍﻳﻦ ﺑﻴﻤﺎﺭﻱ ﺑﻨﺎﺑﺮﺍﻳﻦ ﻫﻴﭻ ﻣﺪﺭﮎ ﻗﺎﻧﻊﮐﻨﻨﺪﻩﺍﻱ ﻭﺟﻮﺩ ﻧﺪﺍﺭﺩ ﮐﻪ ﺗﻌﻴﻴﻦ ﻛﻨﺪ ﺩﺍﺷﺘﻪ ﺑﺎﺷﺪ. ﺑﻨﺎﺑﺮﺍﻳﻦ، ﺑﺮﺭﺳﻲﻫﺎﻱ ﺁﻳﻨﺪﻩﻧﮕﺮ ﺩﺭﺑﺎﺭﻩﻱ ﺍﺣﺘﻤﺎﻝ T-Score ﺧﻄﺮ ﺷﮑﺴﺘﮕﻲ ﺩﺭ ﺟﻮﺍﻣﻊ ﺭﻭﺳﺘﺎﻳﻲ ﺑﺎ ﮐﺪﺍﻡ .ﺷﮑﺴﺘﮕﻲ ﺍﺳﺘﺨﻮﺍﻥ ﺑﺎ ﺩﻭ ﻣﻌﻴﺎﺭ ﻧﺎﻣﺒﺮﺩﻩ ﺗﻮﺻﻴﻪ ﻣﻲﺷﻮﺩ ﻫﻢﺧﻮﺍﻧﻲ ﺩﺍﺭﺩ ﻭ ﺗﻨﻬﺎ ﺑﺎ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ ﺁﻳﻨﺪﻩﻧﮕﺮ ﺩﺭ ﻣﻮﺭﺩ ﻭﻗﻮﻉ ۲۴،۲۵ ﺳﭙﺎﺳﮕﺰﺍﺭﻱ: ﺍﺯ ﻫﻤﻪﻱ ﺍﻓﺮﺍﺩﻱ ﻛﻪ ﺩﺭ ﺍﻳﻦ ﻣﻄﺎﻟﻌﻪ ﺷﺮﻛﺖ ﻛﺮﺩﻧﺪ ﻭ ﻻﺯﻡ ﺑﻪ .ﺷﮑﺴﺘﮕﻲﻫﺎ ﻣﻲﺗﻮﺍﻥ ﺑﻪ ﻧﺘﻴﺠﻪﻱ ﺩﻟﺨﻮﺍﻩ ﺭﺳﻴﺪ ﻫﻢﭼﻨﻴﻦ ﺍﺯ ﻛﺎﺭﻛﻨﺎﻥ ﻣﺮﻛﺰ ﺗﺤﻘﻴﻘﺎﺕ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ ﺫﮐﺮ ﺍﺳﺖ ﺩﺭ ﺍﻳﻦ ﭘﮋﻭﻫﺶ ﻓﻘﻂ ﺟﻤﻌﻴﺖ ﻣﺤﺪﻭﺩﻱ ﺍﺯ ﻳﻚ ﺩﺍﻧﺸﮕﺎﻩ ﻋﻠﻮﻡ ﭘﺰﺷﻜﻲ ﺷﻴﺮﺍﺯ ﻭ ﺍﺯ ﺧﺎﻧﻢ ﺩﻛﺘﺮ ﻣﺮﺿﻴﻪ ﺑﺨﺸﺎﻳﺶ ﻣﻨﻄﻘﻪﻱ ﺭﻭﺳﺘﺎﻳﻲ ﻣﻮﺭﺩ ﺑﺮﺭﺳﻲ ﻗﺮﺍﺭ ﮔﺮﻓﺖ ﻭ ﺑﺮﺍﻱ ﻛﺮﻡ، ﺧﺎﻧﻢ ﺩﻛﺘﺮ ﻫﻠﻦ ﻃﺎﻫﺮﻱ ﻭ ﺧﺎﻧﻢ ﺯﻫﺮﺍ ﮊﻭﻟﻴﺪﻩﭘﻮﺭ ﺗﺸﻜﺮ ﻭ ﺑﻬﺮﻩﺑﺮﺩﺍﺭﻱ ﺳﻮﺩﻣﻨﺪ ﺍﺯ ﺍﻳﻦ ﻣﻌﻴﺎﺭﻫﺎ ﻻﺯﻡ ﺍﺳﺖ ﻣﻄﺎﻟﻌﻪﻫﺎﻱ .ﻗﺪﺭﺩﺍﻧﻲ ﻣﻲﻧﻤﺎﻳﻴﻢ ﺑﻴﺸﺘﺮﻱ ﺩﺭ ﺳﺎﻳﺮ ﻣﻨﻄﻘﻪﻫﺎﻱ ﺭﻭﺳﺘﺎﻳﻲ ﺍﻳﺮﺍﻥ ﺍﻧﺠﺎﻡ ﺷﻮﺩ ﺑﺎ 11. Wang Y, Tao Y, Hyman ME, Li J, Chen Y. References Osteoporosis in China. Osteoporos Int 2009; 20: 1651-62. 1. NOF, National Osteoporosis Foundation. Clin- 12. Looker AC, Waner HW, Dunn WL, Calvo MS, ician’s Guide to Prevention and Treatment of Harris TB, Heyse SP, et al. Update data on Osteoporosis. Washington, DC, NOF, 2009. proximal femur bone mineral levels of US adults. 2. IOF, International Osteoporosis Foundation. Diag- Osteoporos Int 1998; 8: 468-89. nosis of Osteoporosis. 13. Meyer HE, Berntsen GK, Søgaard AJ, Lang- 3. Gordana M. Osteoporosis in men. Journal of the hammer A, Schei B, Fønnebø V, et al. Higher Royal Society of Medicine 2001; 94: 620-3. bone mineral density in rural compared with urban 4. Khosla S. Update in male Osteoporosis. J Clin dwellers: the NOREPOS study. Am J Epidemiol Endocrinol Metab 2010; 95: 3-10. 2004; 160: 1039-46. 5. Ott SM. Osteoporosis in men. N Engl J Med 2008; 14. Kemper HC, Twisk JW, van Mechelen W, Post 359: 868. GB, Roos JC, Lips P. A fifteen-year longitudinal 6. Johnell O, Kanis JA. An estimate of the worl- study in young adults on the relation of physical dwide prevalence and disability associated with activity and fitness with the development of the osteoporotic fractures. Osteoporos Int 2006; 17: bone mass: The Amsterdam Growth And Health 1726–33. Longitudinal Study. Bone 2000; 27: 847-53. 7. Omrani GR, Massoompour SM, Hamidi A, 15. Pongchaiyakul C, Nguyen TV, Kosulwat V, Mardanifard HA, Taghavi SM, Talezadeh P, et al. Rojroongwasinkul N, Charoenkiatkul S, Eisman Bone mineral density in the normal Iranian JA, et al. Effects of physical activity and dietary population: a comparison with American reference calcium intake on bone mineral density and date. Arch Osteoporosis 2006; 1: 29-35. osteoporosis risk in a rural Thai population. 8. Larijani B, Moayyeri A, Keshtkar AA, Hossein- Osteoporos Int 2004; 15: 807-13. Nezhad A, Soltani A, Bahrami A, et al. Peak bone 16. Tan LJ, Lei SF, Chen XD, Liu MY, Guo YF, Xu mass of Iranian population: the Iranian Multic- H, et al. Establishment of peak bone mineral enter Osteoporosis Study. J Clin Densitom 2006; density in Southern Chinese males and its 9: 367-74. comparisons with other males from different 9. Ardawi MS, Maimany AA, Bahksh TM, Nasrat regions of China. J Bone Miner Metab 2007; 25: HA, Milaat WA, Al-Raddadi RM. Bone mineral 114-21. density of the spine and femur in healthy Saudis. 17. Huang QY, Kung AW. Genetics of osteoporosis. Osteoporos Int 2005; 16: 43-55. Mol Genet Metab 2006; 88: 295-306. 10. Wu XP, Liao EY, Zhang H, Dai RC, Shan PF, 18. Ferrari S. Human genetics of osteoporosis. Best Cao XZ, et al. Determination of age-specific bone Pract Res Clin Endocrinol Metab 2008; 22: 723- mineral density and comparison of diagnosis and 35. prevalence of primary osteoporosis in Chinese 19. Broussard DL, Magnus JH .Risk assessment and women based on both Chinese and World Health screening for low bone mineral density in a multi- Organization criteria. J Bone Miner Metab 2004; ethnic population of women and men: does one 22: 382–91. approach fit all?. Osteoporos Int 2004; 15: 349– 60.
- 8. ۱۳۸۹ ﺩﻭﺭﻩﻱ ﺩﻭﺍﺯﺩﻫﻢ, ﺷﻤﺎﺭﻩﻱ ۴، ﺁﺑﺎﻥ ﻣﺠﻠﻪﻱ ﻏﺪﺩ ﺩﺭﻭﻥﺭﻳﺰ ﻭ ﻣﺘﺎﺑﻮﻟﻴﺴﻢ ﺍﻳﺮﺍﻥ ۴۰۰ 20. Araujo A, Travison T, Harris S, Holick M, Turner 23. Kanis J, Borgstrom F, De Laet C, Johansson H , A, McKinlay J. Race/ethnic differences in bone Johnell O, Jonsson B , et al. Assessment of mineral density in men. Osteoporosis International fracture risk. Osteoporosis Int 2005; 16: 581-9. 2007; 18: 943–53 24. Pongchaiyakul C, Rojroongwasinkul N, Chotm- 21. Gu W, Rennie KL, Lin X, Wang Y, Yu Z. ongkol R, Kosulwat V, Charoenkiatkul S, Rajat- Differences in bone mineral status between urban anavin R. Bone mineral density in rural Thai and rural Chinese men and women. Bone 2007; adults living in Khon Kaen province. J Med Assoc 41: 393-9. Thai 2002; 85: 235-44. 22. Larijani B, Moradi Zirkohi A, Hossein-nezhad A, 25. Tenenhouse A, Joseph L, Kreiger N, Poliquin S, Keshtkar A, Kamalian MS, Mojtahedi AR, et al. Murray TM, Blondeau L, et al. Estimation of the Peak Bone Mass Measurement in Iranian Healthy prevalence of low bone density in Canadian Population. Iranian J publ Health 2007, a women and men using a population-specific DXA Supplementary Issue on Osteoporosis 2007; 63-9. reference standard: the Canadian Multicentre Osteoporosis Study (CaMos). Osteoporos Int 2000; 11: 897-904.
- 9. 453/Iranian Journal of Endocrinology and Metabolism Vol 12 No.4 November 2010 Original Article Prevalence of Osteoporosis in Rural Men of Fars Based on Both Local and WHO Reference Data Adine pour A1, Tohidi M1, Dabbaghmanesh M1, Jafari P2, Fattahi M3, Ranjbar Omrani Gh1 1Endocrine and Metabolism Research Center, 2Department of Biostatistic, 3Gastroenterology and Hepatology Research Center Shiraz University of Medical Sciences, Shiraz, I.R. Iran e-mail:hormone@ sums .ac.ir Received: 12/03/2010 Accepted: 04/08/2010 Abstract Introduction: Recently osteoporosis (OP) has emerged as a basic public health problem. It is characterized by low bone mass with micro architectural destruction of bone, resulting in increased bone fractures, morbidity and mortality. Materials and Methods: To evaluate the prevalence of OP using the local reference data of rural males of Fars and to compare it with WHO criteria, a total of 263 male adults, aged between 20-94 yrs, participated in this cross-sectional study. Bone Mineral Density (BMD) was measured by DXA. We utilized a fit curve method to determine the best age range over which to calculate Peak Bone Mass (PBM) and we used regression analysis for association of OP with age and Body mass index (BMI). Results: PBM was observed at the age range of 20-24 years, at the various sites. The prevalence of OP increased with age. It was negatively correlated with BMI and varied dramatically based on local versus WHO criteria. Based on local criteria, prevalence of OP in the lumbar spine, femoral neck and total femur were 3.8%, 24.8% and 14.8%, respectively, and, based on WHO criteria, they were 10%, 6.1% and 24%, respectively. Conclusion: Using local or WHO reference values for evaluation of OP may yield different prevalences. Therefore prospective fracture studies in correlation with the two above reference values are recommended. Keywords: Osteoporosis, Peak Bone Mass, Reference data, WHO