Anatomy of the Abdomen by Sudil Paudyal
•Transferir como PPT, PDF•
128 gostaram•72,574 visualizações


Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Anatomy of the Abdomen by Sudil Paudyal
Semelhante a Anatomy of the Abdomen by Sudil Paudyal (20)
Mais de Sudil Paudyal
Último
Último (20)
Anatomy of the Abdomen by Sudil Paudyal
- 1. By: Sudil Paudyal B.Sc. MIT(51) IOM,MMC 11/01/12 ABDOMEN PRESENTATION BY SUDIL 1
- 2. General Anatomy: The largest cavity of the body, Bounded Anteriorly - by abdominal wall muscles Posteriorly - by the vertebral column and posterior wall muscles Laterally - by lower ribs and parts of muscles of abdominal wall Superiorly - by the diaphragm Inferiorly - by pelvic cavity 11/01/12 ABDOMEN PRESENTATION BY SUDIL 2
- 3. Abdominal walls: Bony support of the abdomen is minimal, consisting only of lumbar vertebrae and portions of the pelvis (the ilium and the pubis). Muscles: Five pairs of muscles form anterior wall: Rectus abdominis External oblique Internal oblique Transversus abdominis Three pairs form the posterior wall: Quadratus lumborum Psoas major Iliacus Linea alba: A very strong midline tendinous cord, extends from xiphoid process to symphysis pubis. Divides the anterior abdominal wall longitudinally into two identical halves. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 3
- 4. Fig: Anterior abdominal wall muscles Fig: Posterior abdominal wall muscles 11/01/12 ABDOMEN PRESENTATION BY SUDIL 4
- 5. Planes and regions: Divided either into four quadrants or nine regions Divided into four quadrants by a transverse and a mid sagittal plane that intersect at the umbilicus. Right Upper Quadrant (RUQ), Right Lower Quadrant (RLQ), Left Upper Quadrant (LUQ), and Left Lower Quadrant (LLQ). 11/01/12 ABDOMEN PRESENTATION BY SUDIL 5
- 6. Divided into nine regions by two transverse and two vertical planes The upper transverse plane - The Transpyloric Plane, Lies midway between suprasternal notch and symphysis pubis, approximately midway between the upper border of xiphisternum and umbilicus. Posteriorly, passes through the body of the first lumbar vertebra; Anteriorly, passes through the tips of the right and left ninth costal cartilages. The lower transverse plane - The Transtubercular Plane, Lies at the level of tubercles of iliac crest anteriorly, and near the upper border of fifth lumbar vertebra posteriorly. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 6
- 7. The two parasagittal (vertical) planes – Lie at right-angles to the two transverse planes. They run vertically, passing through a point midway between the anterior superior iliac spine and the symphysis pubis on each side. These planes divide the abdomen into nine regions: centrally from above to below epigastric, umbilical and hypogastric regions and laterally from above to below right and left hypochondriac, lumbar and iliac regions. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 7
- 8. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 8
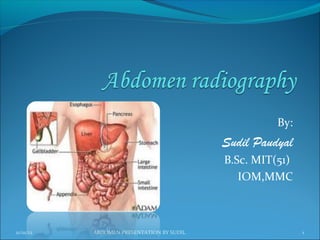
- 9. Contents: contains the greater part of the alimentary tract, some of the accessory organs to digestion, viz. the liver, pancreas and spleen, some of the urinary organs i.e. the kidneys,upper part of the ureters and the suprarenal glands. Most of these structures, as well as the wall of the cavity are more or less covered by an extensive and complicated serous membrane, the peritoneum. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 9
- 10. Fig: organs of anterior part of abdominal cavity 11/01/12 ABDOMEN PRESENTATION BY SUDIL 10
- 11. Fig: organs of posterior part of abdominal cavity 11/01/12 ABDOMEN PRESENTATION BY SUDIL 11
- 12. Peritoneum: The serous membrane related to the viscera of the abdominal cavity. Divided into two layers: Parietal Layer : Lines the body wall and covers the retroperitoneal organs. Visceral Layer : Composed of two parts : Covering of the surface of the peritoneal organs. Mesentery-a double layer of peritoneum that suspends part of the GI tract from the body wall. Peritoneal cavity : The potential space located between the parietal and visceral layers. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 12
- 13. Abdominal Viscera Viscera are classified as: Peritoneal organs - have a mesentery and are almost completely enclosed in peritoneum. These organs are mobile. Retroperitoneal organs - are partially covered with peritoneum and are immobile or fixed organs. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 13
- 14. In a nutshell Major Peritoneal organs: Stomach, Liver and gallbladder, Spleen, Beginning of duodenum, Tail of pancreas, Jejunum, Ileum, Appendix , Transverse colon, Sigmoid colon Major Secondary Retroperitoneal organs: Most of duodenum, Most of pancreas, Ascending colon ,Descending colon , Upper rectum Major Primary Retroperitoneal Organs: Kidney , Adrenal gland, Ureter, Aorta, Inferior venacava, Lower rectum, Anal canal 11/01/12 ABDOMEN PRESENTATION BY SUDIL 14
- 15. Liver: Lies mostly in the right hypochondrium, and protected by rib cage. Divided into two lobes of unequal size by the falciform ligament. Fissures for the ligamentum teres and the ligamentum venosum, the porta hepatis, and the fossa for the gallbladder further subdivide the right lobe into the right lobe proper, the quadrate lobe, and the caudate lobe. Has a central hilus, or porta hepatis, which receives venous blood from the portal vein and arterial blood from the hepatic artery. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 15
- 16. The central hilus also transmits the common bile duct, which collects bile produced by the liver. These structures, known collectively as the portal triad The hepatic veins drain the liver by collecting blood from the liver sinusoids and returning it to the inferior vena cava. Gallbladder : lies in a fossa on the visceral surface of the liver to the right of the quadrate lobe. It stores and concentrates bile, which enters and leaves through the cystic duct. The cystic duct joins the common hepatic duct to form the common bile duct. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 16
- 17. Fig: Liver, turned up to show posterior surface 11/01/12 ABDOMEN PRESENTATION BY SUDIL 17
- 18. Pancreas Most of the pancreas is secondarily retroperitoneal, but the distal part of the tail of the pancreas remains peritoneal . The tip of the tail of the pancreas reaches the hilus of the spleen. Both pancreatic ducts open into the second portion of the duodenum. Spleen a peritoneal organ in the upper left quadrant that is related to the left 9th, 10th, and 11th ribs. Fracture of these ribs may lacerate the spleen. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 18
- 19. Stomach: has a lesser curvature, which is connected to the porta hepatis of the liver by the lesser omentum, and a greater curvature from which the greater omentum is suspended. The cardiac region receives the esophagus. The dome-shaped upper portion of the stomach, which is normally filled with air, is the fundus. The main center portion of the stomach is the body. The pyloric portion of the stomach has a thick muscular wall and narrow lumen that leads to the duodenum. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 19
- 20. Fig: Abd. cavity showing greater and lesser Fig:Longitudinal section of stomach omentum 11/01/12 ABDOMEN PRESENTATION BY SUDIL 20
- 21. Kidneys and ureters: Kidney's Relation to the Posterior Abdominal Wall Both kidneys are in contact with the diaphragm, psoas major, and quadratus lumborum . Right kidney-contacts the above structures and the 12th rib. Left kidney-contacts the above structures and the 11th and 12th ribs Ureter's Relation to the Posterior Abdominal Wall The ureter lies on the anterior surface of the psoas major. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 21
- 22. Fig: Relation of kidneys and ureters to posterior abdominal wall 11/01/12 ABDOMEN PRESENTATION BY SUDIL 22
- 23. Kidneys: A pair of bean-shaped organs approximately 12 cm long. They extend from vertebral level T12 to L3 when the body is in the erect position. The right kidney is positioned slightly lower than the left because of the mass of the liver. Internal structure Within the dense, connective tissue of the renal capsule, the kidney substance is divided into an outer cortex and an inner medulla 11/01/12 ABDOMEN PRESENTATION BY SUDIL 23
- 24. Cortex-contains glomeruli, Bowman's capsules, and proximal and distal convoluted tubules. It forms renal columns, which extend between medullary pyramids. Medulla--consists of 10 to 18 striated pyramids and contains collecting ducts and loops of Henle. The apex of each pyramid ends as a papilla where collecting ducts open. Calyces-the minor calyces receive one or more papillae and unite to form major calyces,of which there are two to three per kidney. Renal pelvis--the dilated upper portion of the ureter that receives the major calyces. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 24
- 25. Fig: cross section of a kidney 11/01/12 ABDOMEN PRESENTATION BY SUDIL 25
- 26. Ureters : are fibro-muscular tubes that connect the kidneys to the urinary bladder in the pelvis. Urinary Bladder: The urinary bladder is covered superiorly by peritoneum. The body is a hollow muscular cavity. The neck is continuous with the urethra. The trigone is a smooth triangular area of mucosa located internally at the base of the bladder. The base of the triangle is superior and bounded by the two openings of the ureters. The apex of the trigone points inferiorly and is the opening for the urethra. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 26
- 27. Fig: Kidneys, Ureters and Bladder 11/01/12 ABDOMEN PRESENTATION BY SUDIL 27
- 28. For any body habitus whether hypersthenic or asthenic, abdominal viscera occupy a lower position: in inspiration compared with expiration; in the erect position compared with the recumbent position; with age and the associated loss of muscle tone. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 28
- 29. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 29
- 30. Radiography: Preparation: Careful preliminary patient preparation of the intestinal and gastric contents is important for a clear view of all the abdominal structures. For non-acute conditions, patient preparation is as follows: (1) Patient placed on a low-residue diet for (2 days) prior to x- ray examination to prevent formation of gas due to excessive fermentation of the intestinal contents (2) Patient should be instructed to take some laxative the night before the examination. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 30
- 31. Exposure technique: In examinations of the abdomen without a contrast medium, it is necessary to obtain maximum soft tissue differentiation throughout its different regions. Because of the wide range in thickness of the abdomen and the delicate differences in physical density between the contained viscera, it is necessary to use a more critical exposure technique than is required to demonstrate the difference in density between an opacified organ and the structures adjacent to it. The exposure factors should thus be adjusted to produce a radiograph with moderate gray tones and less black and white contrast. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 31
- 32. A sharply demonstrated outline of the psoas muscles, lower border of liver, kidneys ribs and spinous processes of the lumbar vertebra are the best criteria for judging the quality of an abdominal radiograph. High mA and shorter exposure times must be used to freeze voluntary and involuntary organ movements (breathing and bowel peristalsis). Exposure is taken on second full arrested expiration (to displace diaphragm upward ) to give a better view of the abdominal structures. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 32
- 33. Immobilization: One of the prime requisite in abdominal examinations is the prevention of movement, both voluntary and involuntary. To prevent muscle contraction, the patient must be adjusted in a comfortable position so that he can relax. A compression band may be applied across the abdomen for immobilization but not compression. The exposure should be made 1-2 sec after suspension of respiration to allow involuntary movement of viscera to subside. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 33
- 34. Radiation protection: Gonadal shields should often be used on males (upper edge of the shield at the symphysis pubis). For females, shields are used only where they could not obscure essential anatomical structures (the lower border of the shield should be at the symphysis pubis). For potential early pregnancy, the ‘10-day Rule’ (the LMP) must always be observed, unless permission has been given by the medical specialist as to ‘ignore’ it, e.g., in the case of an emergency (e.g., trauma), or in case of a female with a removed uterus. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 34
- 35. Radiographic projections: Basic : Antero-posterior – supine (KUB) (so named because it includes the kidneys, ureters and bladder). Alternative: Postero-anterior – prone Supplementary: Antero-posterior –erect Anteroposterior – left lateral decubitus Lateral Lateral- dorsal decubitus Anterior and posterior obliques ( for contrast studies) 11/01/12 ABDOMEN PRESENTATION BY SUDIL 35
- 36. Indications: Bowel obstruction Perforation Renal pathology Acute abdomen Foreign body localization Toxic megacolon Aortic aneurysm Control or preliminary films for contrast studies Detection of calcification or abnormal gas collection 11/01/12 ABDOMEN PRESENTATION BY SUDIL 36
- 37. AP-supine (KUB) Patient position: Patient supine, with the median sagittal plane at right angles Pelvis adjusted so that the ASIS are equidistant from the table Cassette placed longitudinally and positioned so that the symphysis pubis is included Arms placed alongside the trunk or above the head. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 37
- 38. Centering of beam: Vertical central ray directed approx. at the level of a point 1 cm below the line joining the iliac crests. Equipment setting: ( for screen film combination) Kv mA S mAs FFD Film Grid focus size 65 300 0.12 36 100 cm 35 X 43 Yes large cm 11/01/12 ABDOMEN PRESENTATION BY SUDIL 38
- 39. Picture criteria: Whole of abdomen from upper abdomen to symphysis pubis. Lateral abdominal wall and the properitoneal fat layer. Psoas muscle, lower border of liver and the kidneys. Ribs and spinous processes of the lumbar vertebra. Whole of the urinary tract should be visualized. Bowel gas pattern with minimal unsharpness. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 39
- 40. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 40
- 41. PA- prone When kidneys are not of primary interest, PA projection should be used. It reduces patient gonad dose compared to the AP projection Patient position: Patient prone, with median sagittal plane at right angles to the table Arms up beside the head and both legs extended 11/01/12 ABDOMEN PRESENTATION BY SUDIL 41
- 42. CR, equipment setting, picture criteria same as supine projection. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 42
- 43. Lateral: Position of patient: Patient turned onto the side of examination, with hands resting near the head. The hips and knees are flexed for stability. With the MSP parallel to the table, the vertebral column( abt 8 cm anterior to the posterior skin surface) positioned over the midline of the table Immobilization band applied across the pelvis. Cassette centered at the level of iliac crests. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 43
- 44. Centring of the beam: Vertical central ray directed to the centre of the cassette Equipment setting: Kv mA S mAs FFD Film Grid focus size 75 300 0.12 64 100 cm 35 X 43 Yes large cm 11/01/12 ABDOMEN PRESENTATION BY SUDIL 44
- 45. Picture criteria: The prevertebral space along with abdominal aorta Any other intra abdominal calcifications or tumour masses should be clearly visible. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 45
- 46. AP -erect Patient position: Patient stands with the back against the vertical bucky. Patient’s legs separated well apart to maintain a comfortable position. The median sagittal plane is adjusted at right angles and coincident with the midline of the table. The pelvis is adjusted so that the anterior superior iliac spines are equidistant. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 46
- 47. Centring of beam: The horizontal central ray is directed perpendicular to midpoint at the level of iliac crests. Equipment setting: Kv mA S mAs FFD Film Grid focus size 65 300 0.12 36 100 cm 35 X 43 Yes large cm 11/01/12 ABDOMEN PRESENTATION BY SUDIL 47
- 48. Picture criteria: Both domes of diaphragm to ensure that any free air in the peritoneal cavity is demonstrated. Lateral abdominal wall and properitoneal fat Psoas muscle, lower border of liver and kidney shadows Vertebra in center of film. Side identification marker placed properly. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 48
- 49. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 49
- 50. Lateral Decubitus -AP Lateral decubitus is done instead of abdomen erect if patient is unable to stand or sit. Patient position: Patient in lateral recumbent position Elbows and arms flexed and hand resting near head Cassette positioned in vertical bucky against the posterior aspect of the trunk 11/01/12 ABDOMEN PRESENTATION BY SUDIL 50
- 51. Centring of beam: The central ray is directed perpendicular to midpoint at the level of iliac crest with x-ray tube horizontally. Equipment setting: Kv mA S mAs FFD Film Grid focus size 65 300 0.12 36 100 cm 35 X 43 Yes large cm Note: Patient should be placed in lateral decubitus position for 5-10 mins to allow the free air to rise 11/01/12 ABDOMEN PRESENTATION BY SUDIL 51
- 52. Picture criteria: Air fluid levels when an erect abdomen cannot be obtained. Lung area above dome of diaphragm Lateral abdominal wall and properitoneal fat Psoas muscle, lower border of liver and kidney shadows No rotation 11/01/12 ABDOMEN PRESENTATION BY SUDIL 52
- 53. 11/01/12 ABDOMEN PRESENTATION BY SUDIL 53
- 54. Lateral dorsal decubitus (supine): Occasionally, the patient cannot sit or even be rolled on to the side, in which case the patient remains supine and a lateral projection is taken using a horizontal central ray. Patient position: Patient supine Arms raised away from the abdomen and thorax. Cassette positioned vertically against patient’s side 11/01/12 ABDOMEN PRESENTATION BY SUDIL 54
- 55. Centring of the beam: The horizontal central ray is directed to the lateral aspect of the trunk so that it is at right-angles to the cassette and centred to it. Equipment setting: Kv mA S mAs FFD Film Grid focus size 75 300 0.12 36 100 cm 35 X 43 Yes large cm 11/01/12 ABDOMEN PRESENTATION BY SUDIL 55
- 56. Picture criteria: Thorax to the level of mid-sternum and as much of the abdomen as possible. Pre-vertebral space for determining the air fluid levels in abdomen. Lung area above dome of diaphragm, without motion. Patient elevated to demonstrate entire abdomen 11/01/12 ABDOMEN PRESENTATION BY SUDIL 56
- 57. References: Clark’s positioning in radiography, 12th edition Merrill’s atlas of radiographic positions and radiologic procedures, 12th edition Different other books and websites 11/01/12 ABDOMEN PRESENTATION BY SUDIL 57
- 58. THANK YOU 11/01/12 ABDOMEN PRESENTATION BY SUDIL 58