
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Muscles, tendons and will
Semelhante a Muscles, tendons and will (20)
Mais de SonyJames
Último
Último (20)
Muscles, tendons and will
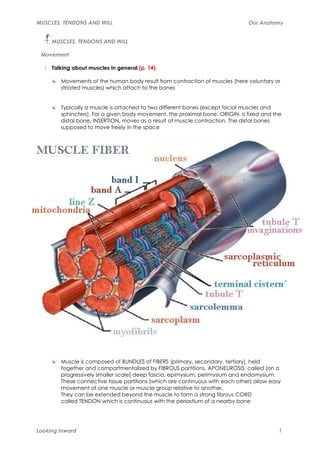
- 1. MUSCLES, TENDONS AND WILL Our Anatomy MUSCLES, TENDONS AND WILL Movement 1. Talking about muscles in general (p. 14) Movements of the human body result from contraction of muscles (here voluntary or striated muscles) which attach to the bones Typically a muscle is attached to two different bones (except facial muscles and sphincters). For a given body movement, the proximal bone, ORIGIN, is fixed and the distal bone, INSERTION, moves as a result of muscle contraction. The distal bones supposed to move freely in the space Muscle is composed of BUNDLES of FIBERS (primary, secondary, tertiary), held together and compartmentalized by FIBROUS partitions, APONEUROSIS, called (on a progressively smaller scale) deep fascia, epimysium, perimysium and endomysium. These connective tissue partitions (which are continuous with each other) allow easy movement of one muscle or muscle group relative to another. They can be extended beyond the muscle to form a strong fibrous CORD called TENDON which is continuous with the periostium of a nearby bone Looking Inward 1
- 2. MUSCLES, TENDONS AND WILL Our Anatomy Individual muscle cells (MYOFIBERS) are extremely long and contain many nuclei. Each cell contains many functional units called SARCOMERES, divided by boundaries called Z lines. Each sarcomere contains thick filaments (made of the protein MYOSIN) and thin filaments (protein ACTINE); the thin filaments are anchored to the Z lines In repose, the myosin and actin filaments are separated. When the muscle is stimulated by a nerve, a series of chemical reactions involving calcium, ATP and magnesium takes place, causing the thin filaments to "slide" along the thick filaments. As a result, the Z lines move closer together, and each individual sarcomere (and therefore the entire muscle) becomes shorter. This is the basis of muscle CONTRACTION, the muscle PULLS from the attached bones Muscle elasticity (p. 15) Besides their (active) ability to CONTRACT, muscles have a (passive) property of ELASTICITY So, a muscle can be stretched to certain point, moving its insertion points further apart, doing the reversed movement of its action. Example: the anterior neck muscles, when they contract, are FLEXORS of the neck. During EXTENSION of the neck, they become stretched. When this happens, because of their elasticity, they tend to return to their initial length, returning the head to its anatomical position 2. Muscle shapes (p. 16) Looking Inward 2
- 3. MUSCLES, TENDONS AND WILL Our Anatomy Muscles attach to bones in several manners: Directly via muscle fibers (usually in broad insertion). Ex.: subscapularis Via an aponeurosis (broad tendon). Ex.: quadratus lumborum Via a regular tendon. Ex.: brachioradialis Sometimes the tendon passes under a fibrous band. Ex.: tibialis anterior A muscle can have several bellies or heads. Ex.: biceps (2 heads), triceps (3 heads), quadriceps (4 heads) Looking Inward 3
- 4. MUSCLES, TENDONS AND WILL Our Anatomy Some muscles can have several origins, which may be in more than one bone (i.e.: the flexor digitorum superficialis originates from both the radius and ulna). Multiple insertions are less common than multiple origins and usually involved finger and toe bones (i.e.: interosseous muscles end, in a complex way, at the 1st phalanx and the extensor tendon of the toe) Muscles have different sizes and shapes: the fiber bundles of muscles are arranged in many shapes Depending on the orientation and attachment of their fibers, muscles may act in one or several directions. Ex.: fibers of rectus abdominis run essentially parallel to each other flexes the trunk; fibers of external oblique arranged like a fan anterior flexion, side-bending or rotation of the trunk LONG muscles are usually kinetic (able to produce visible external motion). SHORT, deep muscles (those inserting on the vertebrae or foot bones) tend to be responsible for precise, small-scale adjustments MONOARTICULAR a muscle that crosses a single joint POLIARTICULAR a muscle that crosses more than one joint. Ex.: rectus femoris (hip and knee) flexor of the hip, extensor of the knee; it will be stretched in situations involving simultaneous extension of the hip + flexion of the knee 3. Muscle contraction (p. 20) Looking Inward 4
- 5. MUSCLES, TENDONS AND WILL Our Anatomy Speaking of a particular movement, the muscle which produces it is called AGONIST, and the muscle which produces the opposite movement is called an ANTAGONIST. Ex.: flexion of the hip, psoas is agonist and gluteus maximus is antagonist SYNERGETIC: different muscles which cooperate to produce the same action. Ex: dorsiflexion of the ankle = tibialis anterior + extensor hallucis longus + extensor digitorum longus. Mutually opposing muscles often function together to fix or stabilize a bone. Ex.: serratus anterior + rhomboids and middle trapezious. By contracting at the same time, they work together to fix the scapula When a muscle contracts, it tends to draw its origin and insertion points closer together. Anything opposing this RESISTANCE. Ex.: brachialis + biceps b., major flexors of elbow. Their action can be opposed by several types of resistance: The weight of the forearm (gravity) The weight of some external object attached to forearm The force of another person pulling on your arm The tension in the muscles that oppose flexion (triceps, elbow extensor), contraction of antagonist muscles Looking Inward 5
- 6. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 6
- 7. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 7
- 8. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 8
- 9. MUSCLES, TENDONS AND WILL Our Anatomy Few extra things Contractions are controlled by the Central Nerve System (CNS), the brain controls the voluntary contractions, while the spinal cord controls the involuntary reflexes Muscle cells (muscular fibers), produce the contractions that move the body parts, including inner organs. The associated connective tissue transports nerve and capillary fibers to the muscle at the same time it wraps it up in bundles or sheaves. Muscles also give shape to the body and generate heat Three types of muscles: Looking Inward 9
- 10. MUSCLES, TENDONS AND WILL Our Anatomy TYPE OF LOCATION ASPECT TYPE OF ACTIVITY STIMULATION MUSCLE Powerful Cylinder-shaped fibers, contraction, Fast It attaches to the Skeletal large, very long, no and intermittent on bone and to the Voluntary by branched, transversely the basal tone; or fascia of the limbs, striated, disposed in serves, above all, the somatic striated body walls and nervous system parallel bundles; many to produce head/neck nuclei in the periphery movement or to resist gravity Involuntary; Branching network intrinsic fibers, many cells linked Powerful stimulation and Muscles of the together, striated contraction, fast, propagation; heart and nearby appearance from its constant and speed and Cardiac portions of the orderly arrangement of rhythmical; pumps strength of the great vessels myofilaments; a single, up the blood from contraction centrally located the heart controlled by nucleus the autonomic nervous system Viscera walls, urinary system, Elongated, spindle- Weak contraction, some respiratory shaped appearance, in slow, rhythmical or passageways, thin sheets or small Involuntary by sustained; serves Smooth certain individual bundles, above all to impel the autonomic reproductive smaller than the other nervous system substances and to organs and blood types, nonstriated; restrain the flow vessels, iris, glands, single central nucleus etc The structural unit of the muscle is the muscle fiber. The motor unit is the functional unit composed by the motoneuron and the muscle fibers enervated by it. When the nerve impulse reaches the motoneuron in the spinal cord, another impulse is generated which determines the simultaneous contraction of all the muscle fibers innerved by that motor unit. The number of muscle fibers in each motor unit goes from one to few hundreds. The number of fibers changes depending on the size and function of the muscle. Movements obey the activation of a progressive number of motor units. Revising: agonists work doing the movement antagonists oppose the action of the agonists; when the agonist contracts, the antagonist relaxes progressively inducing a smooth movement synergists restrain the movement of the articulation inserted between when an agonist crosses more than one joint; these muscles complete the action of the agonist Looking Inward 10
- 11. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 11
- 12. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 12
- 13. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 13
- 14. MUSCLES, TENDONS AND WILL Our Anatomy ATP: adenosine triphosphate is a fundamental nucleotide to obtain cellular energy. Looking Inward 14
- 15. MUSCLES, TENDONS AND WILL Our Anatomy 4. Types of contraction (p. 22) Concentric shortening and eccentric lengthening Concentric contraction When the muscle is stimulated by a nerve and the muscle responds by shortening. Ex.: biceps brachii in the forearm shortens concentrically when lifting up a book, because the origin and insertion points of the muscles are drawn together so the muscle is shorter in length or contracted Eccentric lengthening When we put the book down, we do not ordinarily drop an object we have just lifted, we set it down carefully by slowly extending the elbow, and we accomplish that by allowing the muscle as a whole to become longer while keeping some of its muscles fibers in a state of contraction; in fact can be a bit delicate for the extra work concentrated on those few fibers. Whenever a muscle increases in length under tension while resisting gravity, that movement is eccentric lengthening, typically in actions where we try to slow down a load. It’s usually called lengthening under tension. This “lengthening” can give way to confusion since, although the muscle is lengthening and extending, it’s doing it under pressure and doing no more than going back to its natural resting position We see both actions in most natural daily activities: when walking up a flight of stairs, the muscles lifting us up are shortening concentrically; when walking back down the stairs the same muscles are lengthening eccentrically Ito control our descent. Looking Inward 15
- 16. MUSCLES, TENDONS AND WILL Our Anatomy In Hatha yoga we see both constantly, as when the back muscles shorten concentrically to lift the torso up from a standing forward bend. Then as we slowly lower back down into the bend, the back muscles resist the force of gravity that is pulling us forward, lengthening eccentrically to smooth our descent Isotonic and isometric activity Isotonic Meaning (iso: equal, same - tonic: tone, tension) constant tension. Muscle fibers shorten under a constant load, but this rarely happens in reality. Over time the term has become corrupted to apply generally to exercise that involve movement, usually under conditions of minimal or moderate resistance. Ex.: raising and lowering a book repetitively is an isotonic exercise for the biceps brachii and its synergists. Most athletic activities involve isotonic exercise because they involve movement Isometric Meaning (iso: equal, same - metric: measure/length) constant measure or length. It’s holding still, often under conditions of substantial or maximum resistance. Ex.: holding the book still, neither allowing it to fall nor raising it is an isometric exercise for the same muscles mentioned above. Any and every Hatha yoga posture that we are holding steadily with muscular effort Looking Inward 16
- 17. MUSCLES, TENDONS AND WILL Our Anatomy Relaxation, stretching and mobility The relaxation is the moment when the contraction is over. The different myofibers (actin and myosin) move back into their place and the H zone widens back again. Relaxation is the result of the end of the nerve impulse in the neuromuscular plaque. With certain training we can learn to relax most of our skeletal muscles completely. If a relaxed muscle is gently stretched we can easily go with the stretch provided we have enough flexibility. But if we pull too suddenly or there is any appreciable pain, the nerve system will resist relaxation and keep the muscle tense. Finally, if you allow yourself to remain near your limit of passive but comfortable stretch for a while longer, you may feel the muscles relax again, allowing you to stretch a bit more. This is easier working with partners because stretching on your own is more demanding because you are concentrating on two tasks at the same time: creating the necessary conditions for the stretch, and relaxing into that effort. But the same rules apply, if you go too far and too quickly, pain inhibits lengthening, prevents relaxation and spoils the work Looking Inward 17
- 18. MUSCLES, TENDONS AND WILL Our Anatomy Factors related to SSC (Stretching Shortening Cycle)) The combination of eccentric contractions (when the muscle is active while stretching) and the concentric phase that follows forms a type of natural muscular function called Stretching-Shortening Cycle (SSC). T h e c h a r a c t e r i s t i c o f t h e SSC is that the last contraction of the cycle (concentric phase) is more powerful when immediately preceded by an eccentric contraction than when doing it isolated. Looking Inward 18
- 19. MUSCLES, TENDONS AND WILL Our Anatomy Golgi tendon organ It is a sensory propioceptive receptor placed in the tendons of the skeletal muscles (near musculotendinous junctions). Looking Inward 19
- 20. MUSCLES, TENDONS AND WILL Our Anatomy The body of the Golgi tendon organ is made up of strands of collagen, connected at one end to the muscle fibers, and at the other merge into the tendon proper. When muscles shorten (probably due to the stretch reflex), tension is felt in the point where the muscle is connected to the tendon, place of the Golgi tendon organ. This registers the change in the tension and the proportion of such change and sends signals to the dorsal spine to save this information. When this tension exceeds certain threshold, activates the myotatic reflex than inhibits the shortened muscles and forces them to relax One of the reasons to keep a stretch for a prolonged period of time is that in this way the spindle of the muscle gets used to the new length and reduces its signals. Gradually, its stretching receptors can be trained to allow to increase the length of the muscles Looking Inward 20
- 21. MUSCLES, TENDONS AND WILL Our Anatomy This basic function of the Golgi tendon organ helps to protect the muscles, tendons and ligaments from injures. The reaction of the myotatic reflex is only possible because the signal from the Golgi tendon organ to the spinal cord is powerful enough as to overcome the signal from the skeletal muscles that leads to muscle shortening Looking Inward 21
- 22. MUSCLES, TENDONS AND WILL Our Anatomy When an agonist shortens to cause the desired movement, it usually forces the antagonist to relax. To lengthen, it is easier to stretch a muscle that is relaxed than a muscle that is shortening. Using these situations, when the reciprocal inhibition occurs, we can achieve a more efficient stretch inducing the antagonist to relax during the stretching due to the reduction of the agonists We can also relax any muscle used as synergist by the muscle we are trying to stretch The elongation helps to strengthen the muscle because the capacity of muscle shortening (that is, of generating strength) depends on the initial length. The more the initial muscle length, the better will be the muscle contraction generating more strength (*No olvides estirarte primero) When we have problems to relax, isometric tension-relaxation exercises with reference to the Golgi tendon organ 14-5-10/Ángel Looking Inward 22
- 23. MUSCLES, TENDONS AND WILL Our Anatomy 5. Phasic muscles and postural muscles Restorative alignment Deficient alignment is practically always associated with an imbalance in the surrounding musculature; the maintained bad alignment results in the shortening of some muscles and the constant overstretching of others. When certain muscles are used more frequently than others (at work, doing sports and other activities from daily life), they become more rigid and strong, while the opposite muscles, less used in comparison, become weaker. The consequence is a bad position in the articulation or articulations involved. Most of the therapeutic concepts focus mainly on strengthening the muscles without taking into account the importance of stretching the shortened muscles as well. Looking Inward 23
- 24. MUSCLES, TENDONS AND WILL Our Anatomy Two groups: phasic and postural Phasic muscles, for movement, are the most superficial and tend to be polyarticular. They are basically formed by fast fibers that produce strength but have little resistance. With time and use tend to become shorter and tight Postural muscles, for stability, on the contrary, they are deeper, cross only one joint and are made by slow fibers, good for endurance. They tend to become weaker and to lengthen with time. Their function is to take part in the maintenance of the posture and work against gravity Initially both groups complement each other to stabilize and move; in time the phasic muscles can inhibit the action of the tonic muscles and try to accomplish that function themselves. This inhibition of the stabilizing muscles and the preferential recruitment of the moving muscles is fundamental in the development of imbalance and it is the essence of what wants to be detected and if possible, reverted TONIC MUSCLES PHASIC MUSCLE Neck, shoulder girdle & arm Sternocleidomastoid Rhomboids Pectoralis major Trapezium (ascending) Levator scapularis Trapezium (horizontal) Trapezium (descending) Triceps brachii Biceps brachii Scalenus Trunk Erector spinae, lumbar and cervical region Erector spinae, central thoracic region Quadratus lumborum Abdominal Pelvis- thighs Biceps femoris Vastus medialis Semitendinous Vastus lateralis Semimembranosus Gluteus medius Iliopsoas Gluteus maximus Rectus femoris Gluteus minimus Adductors Gracilis Piriformis Fascia lata tensor Calf & foot Gastrocnemius Tibialis anterior Soleus Peroneus Looking Inward 24
- 25. MUSCLES, TENDONS AND WILL Our Anatomy Common muscle imbalances Many people develop a similar muscular imbalance configuration, almost standardized. While there are many individual variations due to the different activities of the subjects, there is a consistent pattern that results basically from the way we are used to use our postural muscles. There seems to exist a neurological component since these patterns are common and widespread (note from Paola) Upper body patterns neck, middle and upper back, and shoulder girdle show this type of configuration: tension in the extensors of the neck, the upper trapezium and the levator scapularis opposite muscles group: longus capiti and colli (anterior head and neck) and lower trapezium are usually loose and it is necessary to strengthen them in the shoulder the anterior muscles, pectoralis major and minor are usually hypertonic (tense), while the infraspinatus, teres minor, rhomboids and thoracic portion of the spinal erector are inhibited (loose and overstretched) these muscular imbalances end up in very common postural patterns where shoulders move forward and the kyphosis is increased, the head tilts forward and cervical lordosis is lost Lower body patterns there are frequently similar imbalances in the lumbar and pelvic areas. The erector spinae muscles are usually tense and hypertonic, while the abdominal muscles are loose. The flexors of the hip are tight while the inner side of the thigh is not working well with the gluteus maximus, interfering with the complete extension of the hip. It seems that this combination is a factor contributing to the tension of the muscles of the back of the thigh the tight hip flexor muscles will inhibit the posterior ones, which suffer stress during extension. As a result those muscles are overloaded it is impossible to separate the muscles which connect nearby body segments to analyze the possible imbalances correctly, since the alterations in some provoke changes in the position of the bones where the others are inserted Looking Inward 25
- 26. MUSCLES, TENDONS AND WILL Our Anatomy See more about muscular chains Looking Inward 26
- 27. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 27
- 28. MUSCLES, TENDONS AND WILL Our Anatomy 6. Deep back muscles (p.64) Long- splenius capitis and cevicis, erector of the trunk and transversospinalis- and short muscles -interspinalis and intertransverse The long muscle are subdivided in parts depending on its location in the different regions of the vertebral spine Looking Inward 28
- 29. MUSCLES, TENDONS AND WILL Our Anatomy They usually act having the pelvic girdle, the vertebrae and the ribs as a fixed point; the contraction of the muscles pulls from the superior insertions and provokes a movement of the portions of the trunk situated above. In this way, in a standing position with the trunk flexed, the bilateral contraction provokes the extension of the body segment. The hip stays fixed and pulls from the vertebral spine backward, producing extension. If there is unilateral contraction there is flexion to the same side Looking Inward 29
- 30. MUSCLES, TENDONS AND WILL Our Anatomy However, there is no reason for the contrary not to happen, if the upper portions are fixed, these muscles pull the pelvis from the ribs or from the vertebrae. Like a gymnast in the rings, stabilizing the scapula, the shoulder girdle plays the role of an intermediate base and also it is necessary that the deep dorsal muscles, taking as a fixed point the superior vertebrae, pull those below and the pelvic girdle Since the short muscles have a segmental structure and the long muscles are divided depending on their location in relation to the vertebral spine, some weak point can be found in some portion Looking Inward 30
- 31. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 31
- 32. MUSCLES, TENDONS AND WILL Our Anatomy To strengthen these muscles, we need to remember their actions: extension, flexion and rotation of the trunk. It is also important to use the gravitational action with the double purpose of giving variety to the resists and increasing or decreasing their difficulty when necessary. Ex.: when we perform strengthening exercises in decubitus prone (laying facedown) it demands more effort from the extensor musculature of the trunk, since they are working against the gravity force during the whole range of the movement Looking Inward 32
- 33. MUSCLES, TENDONS AND WILL Our Anatomy To lengthen the extensors of the trunk, we need to do the opposite movement, flexion of the trunk, which can be associated with rotations, acting in this way on the oblique fibers. It is important to carry out flexion in the different regions of the vertebral spine: cervical, thoracic and lumbar; if it is performed keeping the trunk extended rotating it around the hip joints, the vertebrae keep their position and the posterior muscles of the trunk stay with same length and those posterior of the hip (joint where the movement takes place) lengthen Looking Inward 33
- 34. MUSCLES, TENDONS AND WILL Our Anatomy 7. Lateral muscle of the lumbar spine: Quadratus lumborum (p. 63) Looking Inward 34
- 35. MUSCLES, TENDONS AND WILL Our Anatomy Posterior and lateral to the vertebral column, helps to hold the weight of the pelvis when we stand on one foot only. A group of fibers of this muscle, which have an oblique direction and insert in the transverse processes of the lumbar vertebrae, provoke a lateral concave curve towards the opposite side. The main function of this muscle is the stability of the lumbar spine, that is why is important the balance in the activity of the quadratus lumborum on both sides of the vertebral spine Its role in extension, hyperextension and in the lateral flexion of the trunk, is affected by the position, or better said, by the changes in the position of the trunk Its action in Trikonasana It pulls from the ribs from the left side towards the hip of the same side (isometric activity) preventing that side from overarching, from rounding, with the consequent loss of space on the right side. Through its action keeps the left side plane and in this way the right side will have room for elongation Looking Inward 35
- 36. MUSCLES, TENDONS AND WILL Our Anatomy 8. Abs and the rest. Anterolateral muscles of the abdomen Looking Inward 36
- 37. MUSCLES, TENDONS AND WILL Our Anatomy They are part of the muscular corset (core) to hold the adequate posture. They are not only in the anterior part of the abdomen, but also reach the ribs and the vertebrae in the back. The transversus, the internal and external obliques and the rectus abdominis form a strong frontal support cushioning the viscera and keeping them in place; at the same time, they are subjected to considerable stress because of the pressure of the viscera against them. If the abdominal wall is weak, the viscera will press more and the muscles will become longer and weaker. Transversus abdominis (p. 92) Looking Inward 37
- 38. MUSCLES, TENDONS AND WILL Our Anatomy It is the deepest one. The only one that due to its biomechanics has repercussions in the vertebral spine. It prevents the collapse of the pelvic base. The structural integrity and balance depend on it. It is much more important than the rectus abdominis because it provides the true essential strength and corrects the pelvic alignment. It attaches below to the inguinal ligament and iliac crest; posteriorly to the thoracolumbar fascia; above to the inner surfaces of the ribs 7-12 (where it interdigitates with fibers of the diaphragm); and anteriorly to the linea alba (a tough fibrous band stretching from the xiphoid process to the symphysis pubis). (The one in red) Action: The contraction of its circular fibers reduces the diameter of the abdominal region. if the vertebrae are fixed collects the abdomen inward if the aponeurosis is the fixed point lumbar lordosis Hands on waist, cough and sneeze and you will find it Internal oblique (p. 93) Looking Inward 38
- 39. MUSCLES, TENDONS AND WILL Our Anatomy Lies between the transversus and external oblique. It is smaller and the average direction of its fibers has the opposite direction of those of the external oblique of the same side. It is attached below to the inguinal ligament and iliac crest; posteriorly to the thoracolumbar fascia; above to the ribs 9-11; and anteriorly to a very broad aponeurosis The average direction of its fibers is anterosuperior, progressively changing until the most anteroinferior fibers are transversal or horizontal. unilateral contraction sidebending or ipsilateral rotation of the spine and ribcage to the same side bilateral contraction compression of the abdomen and assists in flexion of the trunk if both the vertebrae and pelvis are fixed pulls from the ribs down and backward: assists in expiration (Moves the thoracic block in line with the pelvic bock) External oblique (p. 94) Looking Inward 39
- 40. MUSCLES, TENDONS AND WILL Our Anatomy It is external to the other two muscles mentioned above. It is the biggest. It is attached above to the outer surface of ribs 5-12 (where its fibers intertwine with those of the serratus anterior and latissimus dorsi). In front and below it forms a broad aponeurosis ending at (and contributing to) the linea alba and inguinal ligament. The average direction of the fibers is anteroinferior, i.e., perpendicular to those of the internal oblique Action: unilateral contraction side-bending to the same side and contralateral rotation of the spine and ribcage. If the pelvis is the fixed point, pulls from the ribs and vice versa bilateral contraction compresses the abdomen and assists in flexion of the trunk. With the pelvis fixed pulls from the ribs (assists in expiration) The synergic action of the obliques and quadratus lumborum in Trikonasana (tri-angle pose) and other little details The vertical fibers of both obliques assist the quadratus lumborum in pulling from the ribs and pelvis toward each other and in keeping in Trikonasana the up facing side plane instead of arching The obliques act synergetically in the movements of spiral rotation of the trunk: external oblique + the opposite internal oblique (referred to as “same side rotator”). Ex.: Rotation of the trunk to the R with flexion R internal oblique + L external oblique The obliques, with its intertwined diagonal cross-shaped tissues, act as a good fulcrum to rotate the trunk against gravity Many fibers from the external oblique continue into the fibers of the internal oblique of the opposite side. The external oblique acts together with the internal oblique, so contracting the most lateral fibers of the obliques creates inner abdominal pressure which contributes to the expulsion of abdominal contents in defecation or urination. If the diaphragm is relaxed they produce an active expiratory effort If you tend to hyperextend the inferior part of your back the obliques will assist in holding the internal organs and moving them towards the lumbar area with the help of the transversus. Their action helps to lengthen the inferior part of the back, so it is not hyperextended neither overarched Rectus abdominis, 6-pack (p. 95) Looking Inward 40
- 41. MUSCLES, TENDONS AND WILL Our Anatomy It is the most superficial and is located anteriorly, inside a rectus sheath form by the aponeuroses of the three preceding muscles. It runs from the crest and symphysis of the pubis to the xiphoid process and cartilages of ribs 5-7 It takes the pubis closer to the sternum; it is the most direct of the flexors of the trunk and also assists the other three in compressing the abdomen. Active expiration Exercise are usually performed from decubitus supine position (lying on back, facing up), making the most of the gravity force during the whole flexion and extension of Looking Inward 41
- 42. MUSCLES, TENDONS AND WILL Our Anatomy the trunk. Same as in the case of the extensor musculature of the trunk, to strengthen it we need to observe that this muscle extends between the ribs and the pelvic girdle, so we need preferably movements that take the thorax closer to the pelvis or vive versa Wide flexions in the trunk involve the articulation of the hip and the anterior muscles to the hip, NO the intervertebral joints, so it is preferable to make “short” movements, at the level of the cervical, thoracic and lumbar regions of the vertebral spine It is not recommended to do leg-abdominal work because the “psoas paradox” may show up, the inversion of its function, acting as hyperextensor of the lumbar spine. If the abdominal muscles contract at the same time the legs are coming up, there is no forward tilt of the pelvis as a result of the action of the psoas, but if the abdominal muscles are weak, the pelvis tilts forward and the lumbar vertebrae with move away from the floor, increasing the lumbar lordosis, a effect we do not desire. We can perform it not lowering the legs more than 30° Looking Inward 42
- 43. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 43
- 44. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 44
- 45. MUSCLES, TENDONS AND WILL Our Anatomy 9. Deep hip muscles I (p. 208) Group of six muscles: Piriformis, obturator internus and externus, gemellus superior and inferior and quadratus femoris. They go from the pelvis to the greater trochanter. They are covered by the inferior half of the gluteus maximus They are external rotators. They stabilize the hip by straightening and holding the femoral head in the acetabulum Piriformis (p. 209) Originates in the anterior sacrum and goes poster inferiorly (outward and downward), passes under the greater sciatic notch, which forms like a bridge above the muscle, and inserts on the superior surface of the greater trochanter. Connects the sacrum with the femur Action: if the sacrum is fixed laterally rotates the femur and abduction and flexion if the femur is fixed: bilateral contraction contributes to retroversion of the pelvis unilateral contraction medial rotation of the pelvis around the femur The following structures come out of the pelvis through the greater sciatic notch: Location Name Vessels Nerves 2 1 3 Above the piriformis muscle suprapiriformis notch superior gluteal vessels gluteus superior 3 gluteus inferior pudendal inferior gluteal vessels sciatic 2 Below the piriformis muscle infrapiriformis notch medial pudendal artery posterior femoral and vein cutaneous obturator internus quadratus femoris Looking Inward 45
- 46. MUSCLES, TENDONS AND WILL Our Anatomy If it is very voluminous, in its passage through the greater sciatic notch may compress the many vessels and nerves that pass this way. Looking Inward 46
- 47. MUSCLES, TENDONS AND WILL Our Anatomy Sciatic nerve innervates the skin of the leg, the muscles of the back of the thigh and those of the leg and foot. It is the longest and widest single nerve in the human body, the main nerve in the sacral plexus. It originates from the roots L4-S3, although the principal roots come from L5-S1. Occasionally (1-10% of the cases) it goes through the piriformis muscle The piriformis muscle is the main external rotator when the hip is neutral or extended. It is also abductor when the hip is flexed in 90°. If it is a complete flexion it seems to act as internal rotator. Its function is often to restrain a vigorous or fast internal rotation of the hip. The inferior fibers of the piriformis are able to produce a strong force which tends to move the base of the sacrum forward and the vertix of the sacrum backward (nutation) Looking Inward 47
- 48. MUSCLES, TENDONS AND WILL Our Anatomy Piriformis syndrome is a neuromuscular disorder that occurs when the sciatic nerve is compressed or otherwise irritated by the piriformis muscle causing pain, tingling and numbness in the lumbar region, groins, perineum, buttock, hip, back of the thigh, leg and foot. The pain can be chronic and worsens when the piriformis is firmly pressed against the sciatic nerve, as in seating for long periods, the muscle thickens in repose (from having been contracted and shortened actively). This pseudo sciatic of the piriformis is less painful than the true sciatic that originates with a herniated disk at a lumbar level Symptoms are usually associated with spasm of the piriformis or with the compression of the sciatic nerve. Referred pain can be felt in the posterior thigh, most of the lower leg, the entire foot, and part of the pelvis. Decrease of ROM in inner rotation of the same side of the hip In many of the piriformis syndrome cases, there is a rotation of the sacrum towards the same side or towards the contralateral oblique axis, as a result of a compensatory rotation in the lumbar vertebrae in the opposite direction. The rotation of the sacrum often creates the sensation of having a shorter leg on that side Looking Inward 48
- 49. MUSCLES, TENDONS AND WILL Our Anatomy Compensatory and facilitator somatic dysfunctions create advantages in the cervical and thoracic area and pain in the lower back and also stomach disorders and headaches. The ROM of vertebrae T10 and T11decreases, the texture of the tissues from T3 and T4 changes, pain and decrease of ROM on the contralateral side of vertebra C2 and injure on the same side of the occipital-atlas joint Every tension at the end of the spine is transmitted to the legs through the pelvis and hip, and it is precisely there where the piriformis has a protagonist role. In a standing position, it rotates the hip laterally (outward) and moves the thigh away from the center of the body (abduction), creating an excessive tension in the spine that can overload its base, the sacrum bone which is like the foundations of the vertebral spine. If the sacral bone is not in alignment with the iliac bones from both sides, in each stride the sacroiliac joint is jammed, blocked. This joint has a very short articular trajectory, but it is enough to produce a clamp effect in the sacrum, and that tenses excessively the muscle that originates in each of its sides and heads to the hip, and that is no other than the piriformis Looking Inward 49
- 50. MUSCLES, TENDONS AND WILL Our Anatomy In some cases, the muscle can be damaged due to a fall on the buttock. The hemorrhage in and around the piriformis muscle damages the muscle. The piriformis swells up and compresses the sciatic nerve. The injure heals quickly, but the muscle is in spam. The sciatic nerve stays irritated and keeps on being a problem. Finally, the muscle heals, but some of its fibers are substituted by scar tissue. The scar tissue is not as flexible and elastic as the tissue in the normal muscle. The piriformis can be tense and apply a constant pressure on the sciatic nerve Sitting can result difficult. Generally, people with piriformis syndrome do not want to sit down. When they sit they tend to do it on the contralateral buttock and the affected buttock tilting upward. The pain is also aggravated by squatting Weakness, rigidity and general restriction of movement are also frequent in this syndrome. Before stretching the piriformis, the articular capsule of the hip has to be mobilized anterior and posteriorly, to allow a more efficient stretch. The affected leg often rotates laterally (the toes move outward) when the person is relaxed. You can observe it easily when they are lying on the mat The right leg is usually affected alter driving some distance if the foot was in lateral (external) rotation while pressing the gas pedal Looking Inward 50
- 51. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 51
- 52. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 52
- 53. MUSCLES, TENDONS AND WILL Our Anatomy Quadratus femoris (p. 210) It inserts in the lateral ischium, behind the obturator foramen, and runs in a horizontal line laterally (outward), ending up in the posterior aspect of the greater trochanter Action: if Iliac bone fixed lateral rotation of the thigh if the femur is fixed: bilateral contraction contributes to retroversion of the pelvis unilateral contraction medial rotation of the iliac around the femur Obturator internus (p. 210) It arises from the internal surface of the iliac, from the obturator membrane and adjacent portions of the ischium and ilium, its fibers pass posteriorly through the lesser sciatic notch, make a sharp bend around the body of the ischium, where there is a bursa to reduce friction and inserts on the medial aspect of the greater trochanter. It helps to stabilize the hip joints because of its broad origin. Action: if the iliac is fixed it laterally rotates the femur, in flexion and abduction if the femur is fixed: bilateral contraction retroversion of the hip unilateral contraction medial rotation or medial flexion of the iliac. Looking Inward 53
- 54. MUSCLES, TENDONS AND WILL Our Anatomy Gemellus superior and inferior (p. 211) They are like satellites of the obturator internus, inserted above and below its distal borders, end up in the greater trochanter. They reinforce the actions of the obturator internus. Obturator externus (p. 211) It arises from the external surface of the obturator membrane, passes posterior to the femoral neck, and inserts on a fossa on the medial surface of the greater trochanter. Action: if the iliac is fixed is the ideal lateral rotator of the thigh, and assists in flexion and abduction if the femur is fixed: bilateral contraction anteversion of the pelvis unilateral contraction medial rotation or medial flexion of the iliac Obturators and gemelli: the hammock (p. 212) Because of their combined action, they have been compared to a hammock supporting the pelvis from the femur. Observing from the side, the obturator internus and the gemelli run from the greater trochanter in a posteroinferior direction while obturator externus runs anteroinferiorly: if the pelvis is fixed they will pull the femur down relative to the pelvis if the femur is fixed they will lift the pelvis relative to the femur Either way, they tend to pull apart the hip joint on a very small scale. This is a decompressive effect which is quite beneficial for certain painful conditions (e.g., worn-down cartilage). Looking Inward 54
- 55. MUSCLES, TENDONS AND WILL Our Anatomy 10. Deep hip muscles II Iliopsoas (p. 62-213) It is located in the abdominal cavity, running anterior to the pelvis, posterior to the inguinal ligament and inserts on the lesser trochanter (the anterior part of the thigh). There is a bursa to reduce friction where it bends at the anterior pelvis. It is constituted by two portions: psoas major and iliacus. They are often described as a single muscle because they share the same tendon and have the same action on the thigh. But their superior attachments are different: when the femur is fixed, iliacus acts on the pelvis, the psoas on the lumbar spine Looking Inward 55
- 56. MUSCLES, TENDONS AND WILL Our Anatomy Psoas or psoas major arises from the bodies of T12 through L5, and from the arches of fascia which connect the boney parts of the vertebral bodies but do not attach to the intervertebral disks. It goes inferiorly and a little anteriorly towards the internal iliac fossa where is going to meet the iliac portion of the muscle. It inserts on the lesser trochanter action: if the vertebrae are fixed: flexes the hip and works as a weak adductor and lateral rotator if the femur is fixed: bilateral contraction it has been described as a lumbar muscle involved in increasing lordosis, but this polyarticular muscle can have a more complex action on the level of the lumbar spine. Because of its placement on several levels in the convex area of the lumbar spine, this muscle participates in straightening the spine, in combination with the posterior transversospinalis muscles unilateral contraction pulls the lumbar spine into sidebending, flexion and rotation of the side opposite the contraction Looking Inward 56
- 57. MUSCLES, TENDONS AND WILL Our Anatomy Iliacus arises from the entire internal iliac fossa and inserts on the lesser trochanter via a tendon action: if the iliac is fixed action is identical to that of the psoas in flexing the hip with a little adduction and lateral rotation if the femur is fixed: bilateral contraction flexion of the pelvis (the ASIS move forward and downwardly) unilateral contraction flexion of the pelvis and rotation towards the contracted muscle Me gustaría, al menos en los más importantes, ofrecer ejercicios de yoga, posiciones, para estirar o fortalecer el músculo en concreto. Dejo esta nota acá ahora vale? Es para acordarnos jijiji In its path, the iliopsoas is related with important organs: diaphragm, kidneys, ureter, kidney vessels, colon, primitive iliac arteries and external iliac arteries and veins. It has an especially close relationship with the lumbar plexus, which is crossed by the muscle. The iliopsoas is innervated by the lumbar Plexus and femoral nerve Looking Inward 57
- 58. MUSCLES, TENDONS AND WILL Our Anatomy Action: if the vertebrae are fixed flexes the hip, and works as a weak adductor and lateral rotator if the femur is fixed: bilateral contraction participates is straightening the lumbar spine unilateral contraction pulls the lumbar spine into sidebendig, flexion, and rotation of the side opposite the contraction. Looking Inward 58
- 59. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 59
- 60. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 60
- 61. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 61
- 62. MUSCLES, TENDONS AND WILL Our Anatomy LUMBAR PLEXUS Looking Inward 62
- 63. MUSCLES, TENDONS AND WILL Our Anatomy Gluteus minimus (p. 216) A small muscle originating just anterior to gluteus medius and inserting on the anterior aspect of the greater trochanter Its action is similar to that of the anterior fibers of the gluteus medius, but weaker if the iliac is fixed: flexion, abduction and medial rotation of the thigh if the femur is fixed: bilateral contraction anteversion of the pelvis unilateral contraction lateral flexion or lateral rotation of the pelvis Gluteus medius (p. 215) It has a broad origin on the external iliac fossa. Its fibers converge and insert on the lateral aspects of the greater trochanter Action: if the iliac is fixed: its major action is abduction of the hip, but it can also assist in flexion with its anterior fibers and extension with its posterior fibers if the femur is fixed: bilateral contraction it is involved in both anteversion and retroversion of the pelvis, depending on whether the anterior or posterior fibers contract unilateral contraction it acts in lateral flexion of the pelvis, and also, very important, it stabilizes the pelvis during walking or standing on one foot, to prevent it from collapsing to the opposite side Looking Inward 63
- 64. MUSCLES, TENDONS AND WILL Our Anatomy 11. Deep hip muscles III (+ 1 of the hip and knee): The adductors (p. 224) They are a group of five muscles having their bodies on the medial thigh They originate gradually on the pubis and insert on the linea aspera of the femur Action of the group as a whole: If the pelvis is fixed their primary action is adduction of the femur. To a lesser degree they can act from anatomical position as hip flexors or lateral or medial rotators. If the hip is in flexed position they act as extensors. Gracilis (polyarticular) can also flex and medially rotate the knee. If the femur is fixed they are involved in anteversion, medial flexion (sidebending), lateral rotation, or (in the case of gracilis and the posterior portion of adductor magnus) medial rotation of the pelvis These muscles, especially the gracilis, are frequently strained or torn (“pulled groin”) during movements involving sudden or extreme abduction of the thigh Looking Inward 64
- 65. MUSCLES, TENDONS AND WILL Our Anatomy Pectineus Runs from the lateral pubis Adductor brevis Runs from the medial pubis Looking Inward 65
- 66. MUSCLES, TENDONS AND WILL Our Anatomy Adductor longus Originates even more medially on the pubis. It runs anterior to adductor brevis (almost completely covering it Adductor magnus (p. 225) The largest and strongest of the group is really a compound muscle innervated by two different spinal nerves (obturator nerve and sciatic nerve). Two portions: The anterior portion originates from the ischiopubic ramus, runs inferomedially, and has a very broad insertion on the linea aspera The posterior portion originates from the ischial tuberosity, runs straight down, and inserts just above the medial femoral condyle Looking Inward 66
- 67. MUSCLES, TENDONS AND WILL Our Anatomy Gracilis It is a long, thin, superficial, comparatively weak muscles running from the inferomedial pubis vertically down the thigh (medial surface) and inserts on the tibial shaft just below the medial condyle, it’s biarticular, crossing the hip and femur Action of the group as a whole: If the iliac is fixed adduction of the femur, also flexion and lateral rotation If the femur is fixed medial side bending, anteversion and lateral rotation of the iliac (except for the recto interno and the haz vertical from adductor mayor which produce medial rotation) It acts as a flexor when in anatomical position or with the hip extended. If the hip is flexed they become extensors. Looking Inward 67
- 68. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 68
- 69. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 69
- 70. MUSCLES, TENDONS AND WILL Our Anatomy 12. Hip and knee muscles I: The superficial Tensor fasciae latae (p. 229) Gluteus maximus (p. 228) Deltoid gluteus (superficial portion of gluteus maximus and tensor fasciae latae) (p. 229) Looking Inward 70
- 71. MUSCLES, TENDONS AND WILL Our Anatomy 13. Hip and knee muscles II Quadriceps femoris (p. 217) The muscle as a whole is one of the strongest of the body. It has four bodies which converge into a single tendon that inserts on and surrounds the patella and forms the patellar tendon that inserts in the tibia. Their action is extension of the knee Looking Inward 71
- 72. MUSCLES, TENDONS AND WILL Our Anatomy Vastos intermedius it is the deepest, it originates in the upper femoral shaft and its fibers follow the axis of the femur. It is wrapped up in the vastus lateralis and medialis Vasti they arise from either side of the posterior femoral Shaft, wrap around the sides to meet anteriorly: Vastus medialis (internal) and vastus lateralis (external). They give lateral stability to the knee. They are the active complement of the ligaments. They assist in rotation of the tibia and literally pull from the patella. The three vasti can be stretch by full flexion of the knee and hip. Rectus femoris Arises from the anterosuperior iliac spine, and passes superficial to the three vasti to insert on the common tendon. Thus, unlike the vasti, it crosses the hip as well as the knee, acting on both joints If the pelvis is fixed it flexes the hip and extends the knee (e.g., in walking) If the femur is fixed it can act in anteversion of the pelvis Looking Inward 72
- 73. MUSCLES, TENDONS AND WILL Our Anatomy For stretching rectus femoris, the hip must be in extension and the knee in flexion, moving the insertion points away from each other on the pelvic girdle and on the femur or on the leg bones. Looking Inward 73
- 74. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 74
- 75. MUSCLES, TENDONS AND WILL Our Anatomy Sartorius (p. 220) It is a thin muscle, the longest in the body, superficial. It originates from the ASIS, runs medially down the thigh, superficial to the quadriceps and inserts on the superomedial shaft of the tibia It takes part in flexion and abduction Polyarticular muscle: crosses and acts in the hip and knee joint. if the iliac is the fixed point it flexes, laterally rotates and abducts the hip (femur) and flees the knee with the tibia in medial rotation if the femur is fixed: bilaterally anteversion of the pelvis unilaterally anteversion of the iliac, medial rotation and lateral side bending of the pelvis Looking Inward 75
- 76. MUSCLES, TENDONS AND WILL Our Anatomy 14. Hip and knee muscles III: The hamstrings (p. 221) Semitendinosus, semimembranosus and biceps femoris have their origin in the ischial tuberosity and they insert in the tibia and in the head of the fibula They are in the back of the thigh, from the hip to the knee, producing extension of the thigh and flexion of the leg. They are muscles for movement and with time and use they tend to get shorter and harder, especially when we stay daily seated for hour with the legs flexed. And then, when we want to stretch the knees, we curve the lower back. Working to stretch them, with patience and consistency will relieve the inferior part of the back To stretch them, flex the thigh with the leg extended. Here the insertion points move away from each other and the muscles stretch. Equally, wide flexions of the trunk, as Looking Inward 76
- 77. MUSCLES, TENDONS AND WILL Our Anatomy when trying to touch your toes from standing or seated positions, with knees extended, pelvic girdle moving around the femoral head (the hinge), increasing the inclination of the pelvis so the ischial tuberosity move away from the insertion points in the tibia and fibula, provoking the stretch of the muscles. Combine it with the pushing from the centre of your heel in the opposite direction Combined stretching exercises, 30-1-2009/Ruby y amiga When performing poses to stretch them, give yourself a little massage in the back of the knees in the tendons that delimit the popliteal fossa (p.222) Remember, medial rotation of the thigh, sitting bones move away from the heels and muscles in the pelvic floor active pulling, recoiling the coccyx Looking Inward 77
- 78. MUSCLES, TENDONS AND WILL Our Anatomy Semimembranosus and semitendinosus Extension of the femur, flexion and medial rotation of the knee Biceps femoris Extension and flexion and lateral rotation of the knee They are polyarticular muscles, crossing and acting in the hip and knee joints, combining the actions of both joints: if the iliac bone is the fixed point take the femur in extension (specially if the hip is at the beginning of the flexion) if the femur is fixed takes pelvis in retroversion The lack of flexibility in the hamstrings can be responsible of flexions in the lumbar region, and indirectly, of discs ailments in this zone Looking Inward 78
- 79. MUSCLES, TENDONS AND WILL Our Anatomy SHOULDER GIRDLE MUSCLES Includes a big group of muscles divided into two categories: scapulo-thoracic shoulder, which consists of the muscles that mobilize and fix the scapula and clavicle with respect to the thorax scapulo-humeral shoulder, which consists of the muscles that mobilize the humerus and stabilize it with respect with the glenoid cavity of the scapula It is important to highlight that the mobility of the sternoclavicular and acromioclavicular joints allows the scapula to move in various directions, so the glenoid cavity can point in many directions, greatly increasing the ROM of the glenohumeral joint (humerus)); there is a close relation between the movements of the humerus, scapula and clavicle. The position of the scapula, independently of its clavicular relation, obeys the muscular dispositions between this bone and the vertebral spine … So, if from the skeletal-articular point of view there is not a direct relation between the scapula and the vertebral axis, from the functional point of view we have several elements that establish this relation The scapular adductor muscles, i.e., the ones that pull the scapula towards the vertebral spine (mainly the rhomboids and middle fibers from the trapezius) tend to get weak and long due to the posture usually adopted in our daily life where the scapula moves away form the vertebral axis and becomes prominent in the back (winged scapulae). This pattern is reinforced by the shortening of pectoral major Looking Inward 79
- 80. MUSCLES, TENDONS AND WILL Our Anatomy We need to pay especial attention to the adductor muscles, for this, working in pairs can be very useful, where one person is opposing resistance to the movement of adduction of the scapula. To achieve the action of these muscles we can perform movements of the arm that involved the adduction of the scapula, against the resistance of the other person; from horizontal position, with the forearm extended or flexed, extend the arm (moving it backwards) while another person offers resistance to the movement. These exercises have the advantage that, apart from strengthening the scapular adductor muscles they also achieve the elongation of the pectoral major Looking Inward 80
- 81. MUSCLES, TENDONS AND WILL Our Anatomy 15. Shoulder muscles (p. 114) Each scapula, extremely mobile bone floating in the superior part of the back, is a stable connection for the humeral head, stable almost entirely thanks to 5 muscles on each side that keep it in place. Apart from stabilizing the scapula they move it around the surface of the upper back. From 1 to 5, from the deepest to the most superficial: 2 towards the front of the chest: 1. serratus anterior 2. pectoralis minor 3 in the back: 3. rhomboids 4. levator scapulae 5. trapezius All the movements provided by these muscles are crucial for the inversion poses where the superior extremities have to hold the position, and we depend more on strength and flexibility than on strong bones and joints designed to bear the weight of the body The pelvis is connected to the spine by the sacroiliac joints and forms a relatively stable origin from which the muscles can move the thighs while the scapulae themselves take part in the movement of the arms. Therefore, the movements of the scapulae are very important in all inversion and semi-inversion positions Looking Inward 81
- 82. MUSCLES, TENDONS AND WILL Our Anatomy Serratus anterior It is a broad, thin muscle covering the lateral ribcage (lateral superior face of the thorax). Its name is due to its saw-shape. It is formed by 10 muscular bellies. From the surface only the last three inferior bellies are noticeable It originates from the upper ten ribs, we consider 3 levels: upper portion: ribs I and II (converging moderately) middle portion: ribs III to V (diverging) lower portion: ribs VI to X (converging). This portion interweaves with the fibers of the external oblique of the abdomen It inserts along the entire medial border of the scapula. Three levels: upper fibers: superior angle of the scapula, they are ascending and insert on the anterolateral surface of the ribs I and II middle fibers: medial border of the scapula, they are more or less horizontal and insert on the anterolateral surface of the ribs III, IV and V lower fibers: inferior angle of the scapula, they are descending and insert on the anterolateral surface of the ribs VI, VII, VIII, IX and X Looking Inward 82
- 83. MUSCLES, TENDONS AND WILL Our Anatomy Function: If the ribs are fixed it flattens the medial border of the scapula against the ribcage and fixes it against the thorax assisted by the rhomboids Upper fibers: pull the scapula laterally (abduction) and into upward rotation Middle fibers: in actions such as push-ups, the middle fibers of trapezius (adductor) and serratus (abductor) contract simultaneously to stabilize the scapula Lower fibers: together with the lower trapezius depress the scapula moving its inferior angle laterally to allow the elevation of the arms beyond the horizontal There are some fatty layers (gliding planes) separating serratus from the ribcage and from the subscapularis muscle. These increases the mobility of the scapula and are important in many complex movements of the shoulders. If the scapula is fixed the lower fibers lift the middle ribs, acting as inspiratory muscles Looking Inward 83
- 84. MUSCLES, TENDONS AND WILL Our Anatomy Pectoralis minor (p. 116) Deep muscle covered by the pectoralis major It originates from ribs 3-5 and inserts on the coracoid process Actions: if the ribs are fixed pulls the scapula downward and forward, tilting the scapula above the ribcage by lifting the inferior angle upward if the scapula is fixed elevates the ribs acting as an accessory inspiratory muscle Rhomboids (major and minor) (p. 117) Flattened muscles between the spine and the scapula They originate from the spinous process of C7 and T1-T4 and insert on the media border of the scapula Actions: if the spine is fixed adduct the scapula and rotate it downward if the scapula is fixed pull the thoracic vertebrae laterally Looking Inward 84
- 85. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 85
- 86. MUSCLES, TENDONS AND WILL Our Anatomy Levator scapulae (p. 117) It originates from the transverse processes of C1-C4 and inserts on the superior angle of the scapula. Its oblique fibers go from the base of the head in a downward and outward direction Actions: if the spine is fixed elevation and downward rotation of the scapula (glenoid cavity pointing downward) if the scapula is fixed can reinforce the actions of the splenius cervices: bilateral contraction extend the head and cervical spine unilateral contraction sidebending and rotation toward the contracting side. The ROM of the elevation of the scapula is about 10 cm of which this muscle is responsible for 5 of them Looking Inward 86
- 87. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 87
- 88. MUSCLES, TENDONS AND WILL Our Anatomy Trapezius (p. 74-118) Superficial, large, important diamond-shaped muscle which practically covers half of the spine on both sides, running from the base of the cranium (skull) to the very last thoracic vertebra. Origins: upper fibers: on the occiput, nuchal ligament and spinous processes of the cervical vertebrae down to C7. They are overworked in excess in positions such as sitting in front of a computer or driving which involve a prolonged static load from the suspension of the arms neck pain, muscular rigidity, headache middle fibers: on the spinous processes from C7 down to T3 lower fibers: on the spinous processes from T4 down to T12 Insertions: upper fibers: the lateral superior 1/3 border of the clavicle (collarbone) and acromion middle fibers: scapular spine lower fibers: a tubercle at the medial end of the scapular spine Functions: If the spine is fixed: simultaneous contraction of all the fibers adducts the scapula upper fibers elevation and upward rotation of the scapula, traction of the clavicle middle fibers adduction of the scapula. When force needs to be exerted or absorbed by the arm, the middle fibers (adductor) act together with the serratus anterior (abductor) to stabilize the scapula lower fibers depression and upward rotation of the scapula (glenoid cavity pointing upward) If…what does it happen when you move both shoulders forward? And only one? Looking Inward 88
- 89. MUSCLES, TENDONS AND WILL Our Anatomy Between T7 and T12conects with the latissimus dorsi, forming a “diamond” which is an important point in the structure of the vertebral spine, strong and sensitive at the same time. If there is too much rigidity in this point or wrong strength, the access to the deepest muscles becomes difficult and all the work is done by these superficial muscles. On the other hand, if there is mobility and good coordination, it will be a key point for the practice It is the main responsible for keeping the position of the shoulders when we carry weight, that is why the trapezius works quite enough when bearing weight in the arms, below the head as well as above the head. It becomes a very important muscle for maintaining the posture and most of the problems related with having loaded shoulders are due to a bad contraction of this muscle When force has to be exerted or absorbed by the arm, the middle fibers (adductors) work in synergy with the serratus anterior mobilization of the vertebrae of the superior part of the back + relaxation of the upper fibers of the trapezius = PECTORAL STRETCH improves the position of the shoulders, away from the ears, downwardly and laterally (Work it out on the MITRA) Looking Inward 89
- 90. MUSCLES, TENDONS AND WILL Our Anatomy Articular trauma: the general stability of the synovial joints is established by the action of the muscles surrounding them. Excessive stress in the articulations results in strained muscles and tendons or rupture of ligaments and capsules. When the stress is chronic there are degenerative changes. The incorrect patterns of movement are one of the causes of articular dysfunction During activities which involve lifting up the arms the stabilization of the scapula is the key. The superior part of the trapezius and the levator scapulae fix the scapula from above, while the inferior part of the trapezius and the serratus anterior do it from below. The superior muscles are inserted on the cervical spine while the inferior muscles are inserted on the thoracic spine. As the superior fixing muscles are normally excessively active and the inferior ones inhibited, the over-solicitation of the cervical spine in activities with loads or lifting the arms to reach something is common Looking Inward 90
- 91. MUSCLES, TENDONS AND WILL Our Anatomy Tripod exercise from B4L, to stretch especially the upper fibers Exercises to expand the armpits muscles thorax arms 21-8-08/Spid Looking Inward 91
- 92. MUSCLES, TENDONS AND WILL Our Anatomy Within this section we have two more little muscles: Subclavius (p. 116) Small cylinder shaped muscle, it originates on rib I and its cartilage and inserts on the underside of the clavicle Action: Depresses the clavicle and shoulder. It can also stabilize the sternoclavicular joint We have been told that this little muscle could be very useful if humans still walked on all fours. Some people have one, some none, and a few have two What do you think? Who is she/he laughing at? Looking Inward 92
- 93. MUSCLES, TENDONS AND WILL Our Anatomy Sternocleidomastoid (SCM) (p. 116) Long and robust, the largest and most important anterolateral muscle of the neck Origin: on the mastoid process and the curved superior occipital line Insertions: dual insertions on the sternum (cylindrical) and clavicle (flattened), near their junction on the manubrium. In between them we found the Sedillot triangle, which allows an access to the jugular vein In the middle area of the muscle there is a zone where multitude of nerves converge Actions: when the skull is fixed: elevates the sternum and clavicle, assisting in inspiration when the thoracic cage is fixed: Unilateral contraction ipsilateral sidebending and contralateral rotation of the head, as well as extensión Bilateral contraction extension of the head, stressing the cervical lordosis (concave) Looking Inward 93
- 94. MUSCLES, TENDONS AND WILL Our Anatomy Stretching the trapezius and the SCM Sitting on a chair grab with one hand the side of the chair. Flex the neck, tilt the head towards the opposite side to the one to stretch and turn the head towards the side of the stretch, when feeling the tension we know we found the area to be stretched and we hold the posture of the head supporting it with the other hand. To increase the stretch we sift our weight towards the opposite side to the one we are grabbing Moving the scapula with a partner Looking Inward 94
- 95. MUSCLES, TENDONS AND WILL Our Anatomy Looking Inward 95
- 96. MUSCLES, TENDONS AND WILL Our Anatomy 16. Deep glenohumeral (scapulohumeral) muscles of shoulder joint (p. 120) Subscapularis Supraspinatus Infraspinatus (p. 121) Teres minor Rotator cuff muscles (p. 122) Coracobrachialis Long muscle more suitable for movement than for strength is the smallest of the three muscles that attach to the coracoid process of the scapula (the other two, pectoralis minor and biceps brachii) It arises from the apex of the coracoid process in common with the short head of the biceps brachii and inserts by means of a flat tendon on the medial surface of the humeral shaft, near the middle Actions: flexes and adducts the arm at glenohumeral joint (shoulder) Looking Inward 96
- 97. MUSCLES, TENDONS AND WILL Our Anatomy Biceps brachii (p. 123-139) Close to the coracobrachialis. Topographically is connected to the elbow but functionally is very important in the scapulohumeral joint It is a two-headed muscle located on the upper arm. Both heads arise from the scapula and join to form a single muscle belly which is attached to the upper forearm. While the biceps crosses both the shoulder and elbow joints, its main function is at the latter where it flexes the elbow and supinates the forearm. Both these movements are used when opening a bottle with a corkscrew: first biceps unscrews the cork (supination), then it pulls the cork out (flexion) So, two origins and one insertion: proximally (towards the body), the short head of the biceps originates as a tendon from the coracoid process, goes down vertically and becomes a fleshy body the long head originates on the supraglenoid tubercle just above the shoulder joint from where its tendon passes down along the intertubercular groove of the humerus and along the bicipital groove before merging with the body. When the humerus is in motion, the tendon of the long head is held firmly in place in the intertubercular groove by the greater and lesser tubercles and the overlying transverse humeral ligament. During the motion from external to internal rotation, the tendon is forced medially against the lesser tubercle and superiorly against the transverse ligament insertion: The two heads continue downward and form one tendon, which passes anterior to the elbow joint and inserts at the bicipital tuberosity of the radius Looking Inward 97
- 98. MUSCLES, TENDONS AND WILL Our Anatomy Functions: The biceps is tri-articulate, meaning that it works across three joints. The most important of these functions is to supinate the forearm and flex the elbow. These joints and the associated actions are listed as follows in order of importance: proximal radioulnar joint (upper forearm) contrary to popular belief, the biceps brachii is not the most powerful flexor of the forearm, a role which actually belongs to the deeper brachialis muscle. The biceps brachii functions primarily as a powerful supinator of the forearm (turns the palm upwards). This action, which is aided by the supinator muscle, requires the elbow to be at least partially flexed. If the elbow, or humeroulnar joint, is fully extended, supination is then primarily carried out by the supinator muscle humeroulnar joint (elbow) the biceps brachii also functions as an important flexor of the forearm, particularly when the forearm is supinated. Functionally, this action is performed when lifting an object or when performing a biceps curl. When the forearm is in pronation (the palm faces the ground), the brachialis, brachioradialis, and supinator function to flex the forearm, with minimal contribution from the biceps brachii glenohumeral joint (shoulder) several weaker functions occur at the shoulder joint. The biceps brachii weakly assists in forward flexion of the shoulder joint (bringing the arm forward and upwards). It may also contribute to abduction (bringing the arm out to the side) when the arm is laterally rotated. The short head of the biceps brachii also assists with horizontal adduction (bringing the arm across the body) when the arm is medially rotated. Finally, the long head of the biceps brachii, due to its attachment to the scapula, assists with stabilization of the shoulder joint when a heavy weight is carried in the arm Flexed arm in the pronated position (left); with the biceps partially contracted and in a supinated position with the biceps more fully contracted, approaching minimum length (right) Looking Inward 98
- 99. MUSCLES, TENDONS AND WILL Our Anatomy Triceps brachii (p. 123-140) Latin for "three-headed arm muscle" is the large muscle on the back of the upper limb. It is the muscle principally responsible for extension of the elbow joint (straightening of the arm) Origins: Each of the three heads has its own motoneuron subnucleus in the motor column in the spinal cord. The medial head is formed predominantly by small type I fibers and motor units, the lateral head of large type II b fibers and motor units and the long head of a mixture of fiber types and motor units. It has been suggested that each head "may be considered an independent muscle with specific functional roles" the long head, biarticular arises from the infraglenoid tubercle of the scapula the lateral head arises from the lateral posterosuperior shaft of the humerus the medial head (deep head) arises from the posteroinferior humerus. The medial head is mostly covered by the lateral and long heads Insertion: The fibers converge to a single tendon to insert onto the olecranon process of the ulna (though some research indicates that there may be more than one tendon) and to the posterior wall of the capsule of the elbow joint where bursae (cushion sacks) are often found. Parts of the common tendon radiate into the fascia of the forearm and can almost cover the anconeus muscle Looking Inward 99