1. • Kaiser Permanente
• Piedmont Fayette
• Georgia Charitable Care Network
Acknowledgements
Care Pathways - Prevent and Control Chronic Disease Through a Team
Based Approach that Includes Health Education
Saawan Mehta, Marika Roberts MA, Tedra Boyd MSW, Brianna Mavis RN, Vendella DeMoors MA, Sandra Lancaster,
Loida Bonney MD, MPH
Preliminary Results ConclusionIntroduction Methods
Objectives Pictures
• Free clinics provide the necessary role of
filling gaps in healthcare at the community
level and are funded by charitable donations.
• Patients at Fayette Care Clinic (FCC)
represent the most socioeconomically
disadvantaged people in Fayette County.
• Over 63% of our patients are obese or
morbidly obese
• 19% of FCC patients have diabetes and of
those with diabetes, 43% have hemoglobin
A1C values that are outside of the normal
range.
• Over 35% of FCC patients have a diagnosis of
hypertension.
• 36% of our patients have no income, 34%
are below 100% of the federal poverty limit,
and 30% are below 200% of the poverty
limit.
• They are vulnerable to suffer great health
care disparities related to socioeconomic
status.
1) Improve health status in Obesity, Diabetes
and Cardiovascular disease (CVD) through a
care management system modeled after the
National Committee for Quality Assurance
(NCQA) Patient Centered Medical Home
(PCMH) and
2) Strived to lower BMI for 25% of participants
by 5%, to lower A1c by at least 3%, and to bring
the 10-year ASCVD risk to below 5% by
optimizing blood pressure and cholesterol
values.
Based on the preliminary data, the
participants seemed to have not decreased
their BMI, CVD, or A1C. The methodology of
analyzing the data in the future will be
changed. Many of the participants had follow
up visits without attending educational classes
in between. Therefore, the data will be
stratified between patients who had attended
the classes and those that have not. This will
provide a better indication of whether the
educational classes have been helpful in
participants becoming healthier.
Furthermore, because we are still recruiting
for the program, participants have enrolled
within the last 2-3 months and have not
returned for rechecks. Therefore, they could
not be used for our measurements.
Because we are creating the infrastructure
for a program that was not previously available,
the process has been slow. The program shows
potential to be sustainable for our target
population and will ideally continue in the
coming years.
• Many of the participants had registered
within the last 3 months, making it difficult
for one to assess whether the classes have
been helpful.
• The health education classes had a late start
due to the required permission from
Piedmont Fayette, causing participants to
attend classes later than expected.
• Some participants have not been able to
attend their respective classes, due to
external factors, such as lack of
transportation, inability to leave work, or
family constraints.
Limitations
• Patients will also have increased access to
providers and the interdisciplinary care
team via same day appointments and
after-hours telephone service.
• 84 total participants
• 100% of participants have set 2 or more
goals
• We have offered 8 nutrition classes
• 27 have had 1 class
• 14 have had 2 classes
• 8 have had 3 classes
• 5 have had 4 classes
• 3 have had 5 classes
• 36 participants are identified as diabetic
• 14% have improved A1c
• 39% of the participants had an acceptable
10 year ASCVD risk of 5% or less
• 72% had improvements in the
ASCVD scores
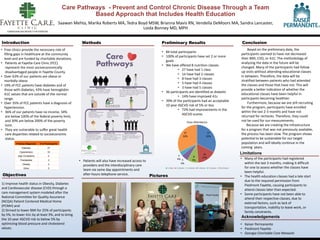
27
32%
14
17%8
9%5
6%
3
4%
27
32%
Class Attendance
1 class 2 classes 3 classes 4 classes 5 classes No classes
Primary Diagnosis # of Participants
Diabetes 37
Hypertension 33
High Cholesterol 5
Prediabetes 2
Obesity 2
Other 5