Stenosis vs risk
•Transferir como PPT, PDF•
0 gostou•262 visualizações

SHAPE Society

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (19)
Destaque
Destaque (19)
Semelhante a Stenosis vs risk
Semelhante a Stenosis vs risk (14)
Mais de Society for Heart Attack Prevention and Eradication
Mais de Society for Heart Attack Prevention and Eradication (20)
Último
Último (20)
Stenosis vs risk
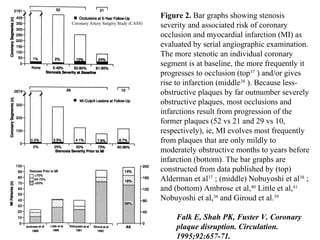
- 1. Figure 2. Bar graphs showing stenosis severity and associated risk of coronary occlusion and myocardial infarction (MI) as evaluated by serial angiographic examination. The more stenotic an individual coronary segment is at baseline, the more frequently it progresses to occlusion (top37 ) and/or gives rise to infarction (middle38 ). Because less- obstructive plaques by far outnumber severely obstructive plaques, most occlusions and infarctions result from progression of the former plaques (52 vs 21 and 29 vs 10, respectively), ie, MI evolves most frequently from plaques that are only mildly to moderately obstructive months to years before infarction (bottom). The bar graphs are constructed from data published by (top) Alderman et al37 ; (middle) Nobuyoshi et al38 ; and (bottom) Ambrose et al,40 Little et al,41 Nobuyoshi et al,38 and Giroud et al.39 Falk E, Shah PK, Fuster V. Coronary plaque disruption. Circulation. 1995;92:657-71. Coronary Artery Surgery Study (CASS)
- 2. Coronary Artery Surgery Study (CASS) stenosis severity and progression to occlusion
- 3. Stenosis severity and progression to MI
- 4. Falk E, Fuster V. Atherogenesis and its determinants. In: Hurst’s The Heart. McGraw-Hill, NY 2001
- 5. Coronary Artery Surgery Study (CASS)
- 8. Significance of spontaneous obstruction of high degree coronary artery stenoses between diagnostic angiography and later percutaneous transluminal coronary angioplasty. Danchin N, Oswald T, Voiriot P, Juilliere Y, Cherrier F. Among 265 patients with severe coronary artery stenoses amenable to percutaneous transluminal coronary angioplasty, 13 (5%) developed new total coronary occlusion of the vessel to be dilated during the period between diagnostic coronary angiography and repeat coronary angiography at the time of the operation. Time from diagnostic to "therapeutic" angiography (76 +/- 74 vs 31 +/- 31 days, p less than 0.0001), degree of coronary stenosis on diagnostic angiography (85 +/- 7 vs 80 +/- 8%, p less than 0.05) and impaired coronary flow distal to the narrowing (Thrombolysis in Myocardial Infarction grade 2: 38 vs 10%, p less than 0.01) were the only variables related to the occurrence of spontaneous coronary occlusion. The clinical course of the patients who developed new total coronary occlusion was remarkably favorable. Twelve of the 13 patients had unchanged or improved anginal symptoms. The electrocardiogram at rest remained unchanged in 11 patients and there was no transmural myocardial infarction. Eight patients had 2 ventriculograms and the mean ejection fraction remained unchanged (only 2 patients had greater than 5% decrease in ejection fraction between the 2 examinations). Spontaneous occlusion of high degree coronary artery stenoses is not unusual and is usually well tolerated, presumably due to the development of collateral circulation. Am J Cardiol. 1989;63:660-2.