Coronary Aneurysms
•Transferir como PPTX, PDF•
7 gostaram•1,841 visualizações

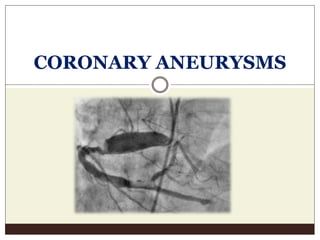
coronary Aneurysms closest differential diagnosis is ectasia

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Coronary Aneurysms
Semelhante a Coronary Aneurysms (20)
Mais de Praveen Nagula
Mais de Praveen Nagula (20)
Último
Último (20)
Coronary Aneurysms
- 2. Intr0duction Aneurysmal coronary artery disease is seen in 0.3-5% of patients undergoing CAG, Giant aneurysms having a prevalence of 0.02% - 2.0% Localised luminal dilation measuring atleast 1.3-2 times the diameter of a normal, adjacent reference segment. Giant Anuerysms – no universal definition - >20mm,40 mm 0r four times the reference vessel diameter have all been proposed as definitive giant aneurysms in literature. Cohen P, O’Gara PT. Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev 2008;16(6):301-4. Nichols L, Lagana S, Parwani A. Coronary artery aneurysm: a review and hypothesis regarding etiology. Arch Pathol Lab Med 2008;132(5):823-8. Morita H, Ozawa H, Yamazaki S, Yamauchi Y, Tsuji M, Katsumata T, Ishizaka N. A case of giant coronary artery aneurysm with fistulous connection to the pulmonary artery: a case report and review of the literature. Intern Med 2012;51 (11):1361-6. Keyser et al (2012) - A compilation of 28 cases of >50 mm over a period of 49 years
- 3. Etiology Atherosclerosis (most common cause ) Takayasu arteritis Kawasaki disease Ehler Danlos syndrome,Marfan syndrome,Polyarteritis Nodosa Fibromuscular dysplasia SLE,Behcet’s disease Trauma Syphilitic aortitis Congenital Secondary to Percutaneous interventions – angioplasty, atherectomy, stenting Cohen P, O’Gara PT. Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev 2008;16(6):301-4.
- 4. Pathogenesis Disruption of the intima and media on the histology. Inherent defect in the vessel wall can predispose atherosclerosis to aneurysm formation. Media is weakened in areas of marked atherosclerosis with decrease in elasticity – decreased stress intolerance to the intraluminal pressure – dilation of the vessel. Delayed reendothelization Hypersensitivity reactions Residual non healing dissections High pressure balloon inflations Percutaneous interventions Chrissoheris MP, Donohue TJ, Young RS, Ghantous A. Coronary artery aneurysms. Cardiol Rev 2008;16(3):116-23. Kelley MP, Carver JR. Coronary artery aneurysms. J Invasive Cardiol 2002;14(8):461-2.
- 6. Natural History Usually Asymptomatic Presentation can be with angina, sudden death, tamponade, congestive heart failure. Rarely as SVC syndrome, mediastinal mass Sequelae – thrombus formation, embolization, fistula formation, rupture. Can produce mid-diastolic murmur in 3rd left ICS Approx. 25% of patients with a giant CAA will have an associated coronary fistula. (Moritia et al,2011) Cohen P, Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev 2008;16(6):301-4. Falsetti HL, Coronary artery aneurysm. A review of the literature with a report of 11 new cases. Chest 1976;69 (5):630-6. Mata KM, Coronary artery aneurysms: an update. In:Lakshmanadoss U, editor. Novel strategies in ischemic heart disease. InTech; 2012. p. 381-40 Zoneraich S, Giant coronary artery aneurysm. The cause of middiastolic murmur and bulging of the left cardiac border. JAMA 1975;231(2):179.
- 7. Management Surgical correction is the preferred treatment. Aneurysmal ligation with distal bypass grafting Isolated coronary artery bypass grafting Anuerysm plication Saphenous venin patch repair of the aneurysm. Antiplatelet or anticoagulants or both – to decrease the risk of thrombus and embolization. PTFE covered stents > 10 mm size aneurysms –high restenosis. Cohen P, Coronary artery aneurysms: a review of the natural history, pathophysiology, and management. Cardiol Rev 2008;16(6):301-4. Chrissoheris MP, Coronary artery aneurysms. Cardiol Rev 2008;16(3):116-23. Szalat A, Use of polytetrafluoroethylene- covered stent for treatment of coronary artery aneurysm. Catheter Cardiovasc Interv 2005;66(2):203-8.