
Recomendados
Basic Needs Form Sheet
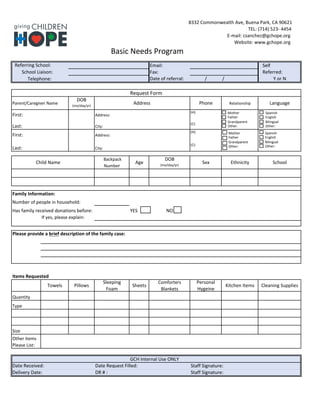
- 1. 8332 Commonwealth Ave, Buena Park, CA 90621 TEL: (714) 523- 4454 E-mail: csanchez@gchope.org Website: www.gchope.org Basic Needs Program Referring School: Email: Self School Liaison: Fax: Referred: Telephone: Date of referral: / / Y or N Request Form Parent/Caregiver Name DOB (mo/day/yr) Address Phone Relationship Language First: Address: (H): Last: City: (C): First: Address: (H): Last: City: (C): Child Name Backpack Number Age DOB (mo/day/yr) Sex Ethnicity School Family Information: Number of people in household: Has family received donations before: YES NO If yes, please explain: Please provide a brief description of the family case: Items Requested Towels Pillows Sleeping Foam Sheets Comforters Blankets Personal Hygeine Kitchen Items Cleaning Supplies Quantity Type Size Other items Please List: GCH Internal Use ONLY Date Received: Date Request Filled: Staff Signature: Delivery Date: DR # : Staff Signature: Mother Father Grandparent Other: Mother Father Grandparent Other: Spanish English Bilingual Other: Spanish English Bilingual Other:
- 2. 8332 Commonwealth Ave, Buena Park, CA 90621 TEL: (714) 523- 4454 E-mail: csanchez@gchope.org Website: www.gchope.org Programa de Necesidades Básicas Referring School: Email: Self School Liaison: Fax: Referred: Telephone: Date of referral: / / Y or N Formulario de Solicitud Nombre del Padre/Tutro FDN (mes/dia/año) Dirección Teléfono Relación Idioma Primer: (H): Apellido: (C): Primer: Dirección: (H): Apellido: Ciudad: (C): Nombre del Niño Número de Mochila Edad FDN (mes/dia/año) Sexo Etnia Colegio Información Familiar: Número de personas en el hogar: Esta familia ha recibido donaciones anteriormente: SI NO En caso afirmativo, por favor explique: Por favor proporcione una breve descripción del caso de la familia: Artículos Solicitados Toallas Almohadas Colchon de Esponja Sábanas Colcha Covija Producto de higiene Artículos de Cocina Artículos de limpieza Cantidad Tipo Tamaño Alguna otra necesidad: GCH Internal Use ONLY Date Received: Date Request Filled: Staff Signature: Delivery Date: DR # : Staff Signature: Madre Padre Abuelo Otror: Madre Padre Abuelo Otro: Español Inglés Bilingüe Otro: Español Inglés Bilingüe Otro: