

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Anatomy Reproductive System
Semelhante a Anatomy Reproductive System (20)
Mais de MarkFredderickAbejo
Mais de MarkFredderickAbejo (20)
Anatomy Reproductive System
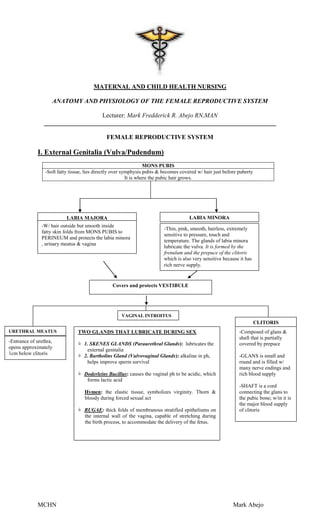
- 1. MATERNAL AND CHILD HEALTH NURSING ANATOMY AND PHYSIOLOGY OF THE FEMALE REPRODUCTIVE SYSTEM Lecturer: Mark Fredderick R. Abejo RN,MAN __________________________________________________________________________ FEMALE REPRODUCTIVE SYSTEM I. External Genitalia (Vulva/Pudendum) MONS PUBIS -Soft fatty tissue, lies directly over symphysis pubis & becomes covered w/ hair just before puberty It is where the pubic hair grows. LABIA MAJORA LABIA MINORA -W/ hair outside but smooth inside -Thin, pink, smooth, hairless, extremely fatty skin folds from MONS PUBIS to sensitive to pressure, touch and PERINEUM and protects the labia minora temperature. The glands of labia minora , urinary meatus & vagina lubricate the vulva. It is formed by the frenulum and the prepuce of the clitoris which is also very sensitive because it has rich nerve supply. Covers and protects VESTIBULE VAGINAL INTROITUS CLITORIS URETHRAL MEATUS TWO GLANDS THAT LUBRICATE DURING SEX -Composed of glans & shaft that is partially -Entrance of urethra, 1. SKENES GLANDS (Paraurethral Glands): lubricates the covered by prepuce opens approximately external genitalia 1cm below clitoris 2. Bartholins Gland (Vulvovaginal Glands): alkaline in ph, -GLANS is small and helps improve sperm survival round and is filled w/ many nerve endings and Doderleins Bacillus: causes the vaginal ph to be acidic, which rich blood supply forms lactic acid -SHAFT is a cord Hymen: the elastic tissue, symbolizes virginity. Thorn & connecting the glans to bloody during forced sexual act the pubic bone; w/in it is the major blood supply RUGAE: thick folds of membranous stratified epitheliums on of clitoris the internal wall of the vagina, capable of stretching during the birth process, to accommodate the delivery of the fetus. MCHN Mark Abejo
- 2. II. Internal Genitalia ORGAN FUNCTIONS STRUCTURE NOTES Divisions of the Uterus Layers of the Uterus: Pear shape muscular organ which has I. Cervix : lowest portion , 1/3 of the 1. Endometrium: Uterus three(3) main total uterus inner layer, most functions vascular, 1. receive the ova External Os: where the nurse obtain SHED DURING from the fallopian the Pap Smear to the MENSTRUATION.THE tube SQUAMOCOLUMNAR JUNCTION NON-PREGNANT 2. provide a place for cells. This is where the cerclage is UTERUS implantation of the done for incompetent cervix. ova 2. Myometrium: 3. Nourishment for Namely: LARGEST PORTION fetal growth. A. Shirodkar Barter Suture- permanent EXPELS THE FETUS closure of the internal cervical os, DURING THE BIRTH until the 38th week after which is PROCESS. The part separated – TREATMENT FOR that contracts during INCOMPETENT CERVIX and hemorrhage. Prevents PREVIOUS ABORTION. hemorrhage. B. Mc Donalds or Purse String Cerclage of the external os: usually 3. Perimetrium: Normal spontaneous delivery will be Outer most layer. Aids done for the patient. for support & added strength. II. Isthmus: shortest portion of the uterus, the portion that is cut when the fetus is delivered during cesarean birth. III. Fundus: Upper segment, this is the most vascular, the portion also where palpation is done. Also touching it by the tip of the fingers during contraction is the best method to determine the intensity of contractions during labor. Bandl’s Ring ( Pathological Retraction Ring): seen in Prolonged Labor or Dystocia MCHN Mark Abejo
- 3. Fallopian Site of fertilization of 4 Parts of the Fallopian tubes Fallopian tubes tubes the ovum with perm 1. Interstitial : lies within the uterine transport the ova from wall the ovaries to the 2. Isthmus: the portion that is cut or uterus. sealed in TUBAL LIGATION ( site for sterilization) 3. Ampulla: where fertilization occurs , this is also the LONGEST portion, frequent site for ectopic pregnancy. 4. Infundibular: covered by the Fimbriae cells that help guide the ova to the Fallopian Tube. Ovaries Ovulation (the release Pair of follicle containing organs on The ovaries lie in the of an ovum); Steroid the other side of the uterus upper pelvic cavity. hormone production Ovaries: 4 by 2 cm in diameter, 1.5 cm thick. Responsible for the production, Maturation, and discharge of ova Secretion of estrogen and progesterone Cortex of the Ovaries; developing and graafian follicles are found here. Vagina Organ for coitus; Tube extending from the introitus to Fibromuscular organ Birth canal; Conduit cervix lined with mucus for menstrual flow. membrane III. THE PELVIS A. Structures 1. Two Os Coxae or Innominate Bones- it is made up of: a. Ilium- is the upper, extended part which has a curved upper border called Iliac Crest. b. Ischium- is the under part which when sitting, the body rests on the ischial tuberosities and an important landmark is the ischial spines. c. Pubis- is the front part that joins to form an articulation of the pelvis called the Symphysis Pubis. 2. Sacrum- a wedge-shaped that forms the back part of the pelvis that consists of 5 fused vertebrae, the first having a prominent upper margin called the Sacral Promontory; it articulates with the ilium and sacroiliac joint. 3. Coccyx- is the lowest part of the spine with a degree of movement between the sacrum and coccyx which is made possible by the third articulation of the pelvis called Sacrococcygeal joint which allows room for delivery of the fetal head B. Divisions 1. False Pelvis- the superior half formed by the ilia offers landmarks for pelvic measurements; it supports the growing uterus during pregnancy and directs the fetus into the true pelvis near the end of gestation. 2. True Pelvis- the inferior half formed by the pubes in front, the ilia and the ischia on the sides and the sacrum and coccyx behind; it is made up of three parts: a. Inlet- the entrance way to the true pelvis wherein its transverse diameter is wider than its anteroposterior diameter, thus Transverse diameter = 13.5 cm Antero-posterior diameter = 11 cm Right and left oblique diameter = 12.75 cm b. Cavity- the space between the inlet and outlet c. Outlet- the inferior portion of the pelvis bounded in the back by the coccyx, on the sides by the ischial tuberosities and in front by the inferior aspect of the symphysis pubis and the pubic arch; its anteroposterior diameter is wider than its transverse diameter C. Types 1. Gynecoid- “normal” female pelvis where inlet is well rounded forward and back; it is most ideal for childbirth. 2. Anthropoid- transverse diameter is narrow, AP diameter is larger than normal. 3. Platypelloid- inlet is oval, AP diameter is shallow. 4. Android- “male” pelvis where inlet has a narrow, shallow posterior portion and pointed anterior portion MCHN Mark Abejo
- 4. D. Types of Pelvic Ligaments 1. Round: remain lax during non-pregnancy & become HYPERTROPHIED & elongated during pregnancy. 2. Cardinal: chief uterine supports 3. Broad ligaments: drapes over the fallopian tubes, uterus & ovaries D. Measurements 1. External- suggestive only of pelvic size a. Intercristal- distance between the middle points of the iliac crests with an average= 28 cm. b. Interspinous- distance between the anterosuperior iliac spines with an average= 25 cm. c. Intertrochanteric- distance between the trochanters of the femur with an average= 31 cm. d. External Conjugate or Baudelocque’s- the distance between the anterior aspect of the symphysis pubis and depression below L5 with an average= 18-20 cm. 2. Internal- gives the actual diameter of the inlet and outlet a. Diagonal Conjugate- distance between the sacral promontory and inferior margin of the symphysis pubis with an average= 12.5 cm. b. True Conjugate or Conjugata Vera- distance between the anterior surface of the sacral promontory and the superior margin of the symphysis pubis; it is very important measurement because it is the diameter of the pelvic inlet with an average=10.5-11 cm. c. Bi-ischial diameter or Tuberischii- transverse diameter of the pelvic outlet and measured at the level of the anus with an average= 11 cm. MALE REPRODUCTIVE SYSTEM External Features: 2 Erectile Tissues in the penis: a. Corpus cavernosa b. corpus spongiosum Internal Features: Epididymis: totals 20 ft. WHERE SPERMS ARE STORED Vas / Ductus Deferens: carries the sperm to the inguinal canal Seminal Gland / Vesicle: Secretes SEMEN Prostrate Gland: secretes SEMEN also. Cowpers Gland/ Bulbo-urethral: secretes also semen SEMEN sources: 1. Prostrate gland : 60% 2. Seminal vesicles : 30% 3. Epididymis : 5% 4. Cowpers : 5% MCHN Mark Abejo
- 5. Accessory Structures Mammary Gland III. Mammary Glands MAMMARY GLANDS -2 mammary glands located on each side of chest wall -Each breast 15-20 lobes containing clusters of ALVEOLI ACINI DUCTULES NIPPLES -Saclike end of -Exit alveoli & join -Sinuses merge into the glandular to form larger canals openings on nipple system LACTIFEROUS -Lined both w/ DUCTS epithelial cells -During lactation, that secrete milk flows to the colostrum( alveoli and then thru which is rich in the duct system IgA) & milk & further going to the w/ muscles that balloon like storage expel milk sacs called LACTIFEROUS SINUSES MCHN Mark Abejo
- 6. Female Reproductive Hormones HORMONES Lutenizing Estrogen Follicle Stimulating Hormone -Produce from ovaries, Hormone -When follicle is adrenal cortex, and Progesterone *Stimulates ripe and mature, placenta *Produce from corpus Graafian follicle to triggers follicular -Assists in maturation of luteum, placenta mature and resulting rupture and release Graafian follicle -Secretes thick/viscous in increase levels of of ovum -Stimulates thickening of cervical secretions. estrogen -Peaks at 16-18 endometrium. hours before Other functions A. Preparation of the ovulation. uterus to receive a -stimulates a. Contracts smooth fertilized ovum ovulation & muscles Inhibits the B. Decrease uterine development of secretion of FSH motility/ corpus luteum b. Responsible for the contractility during increase vaginal pregnancy secretion in the vagina C. Increases basal (LEUKORRHEA) metabolism c. Thickens the D. Enhances endometrium placental growth d. SUPPRESSES THE E. Stimulates the FSH & Prolactin dev’t of acini cells e. Responsible for the in the dev’t of 2ndary sex breast(major cells characteristics in for breast milk) females Increase the f. Stimulates uterine endometriums contractions & supply of smuscular peristalsis glycogen, oxygen of the fallopian tubes & amino acids for for the passage of the maintaining ovum to the uterus. pregnancy g. Mildly increases Na & water reabsorption h. Stimulates LH secretion & responsible for the production of cervical mucus associated in ferning & spinnbarkeit LUTENIZING HORMONE AND ESTROGEN peak immediately before ovulation Most women ovulate two weeks before the beginning of the next period. Other Reproductive Hormones 1. Lactogenic Hormone (Prolactin) -Stimulates lactation 2. Melanocyte Stimulating Hormone -Responsible for the linea nigra & chloasma in pregnancy -Secreted by the anterior pituitary hormone MELANOTROPIN -Will end on the 2nd month of pregnancy 3. Human Chorionic Gonadotropin -Increases in nausea and vomiting Responsible for Hyperemesis Gravidarum MCHN Mark Abejo
- 7. MENSTRUATION Menarche: 1st menstrual period, usually age 12, but may begin as early as 9. Menopause: cessation of menstrual cycle that occurs normally from 40 & 55 y.o. Menstrual Cycle: 1. Menstrual Phase ( 1 – 14 days) -Corpus luteum dies. -Progesterone & Estrogen vanishes- triggers/stimulate the production of FSH. -Endometrium degenerated/ sheds- menstruation occurs. Sexual intercourse during menstruation is not harmful. 2. Proliferative Phase- Estrogen Phase ( 6 – 14 days) Graafian Follicle: Estrogen Anterior Pituitary Gland secretes FSH stimulates the development of the Graafian follicle (secretes Estrogen) suppresses FSH & stimulates LH LH stimulates ovulation Increase Estrogen kills/decreases FSH 3. Secretory Phase (15 to 21 days) Progesterone Phase (Corpus Luteum: Progesterone) Other Books it is called: Luteal Phase After Ovulation-----release of mature ovum from the Graafian follicle----- Graafian Follicles die and replaced by Corpus Luteum-----secretes progesterone Functions of Progesterone: 4. Pre-Menstrual Phase (22 days to 28 days) -If fertilization does not occur, corpus luteum begins to die -Progesterone & Estrogen decreases -Endometrium degenerates -Menstruation stops during pregnancy because there is decrease secretion of hormones by the ovary. OVARIAN CYCLE (ACORDING TO HORMONAL ACTIVITY) 0 7 14 21 28 DEVELOPING FOLLICLES OVULATION CORPUS LUTEUM LUTEAL REGRESSION FOLLICULAR PHASE LUTEAL PHASE Ovarian follicles mature under influence -mittelshmerz of FSH and estrogen -cervical changes LH surge causes ovulation -increase BBT ENDOMETRIAL/UTERINE CYCLE (Described by varying thickness of the endometrium) MENSTRUAL PROLEFERATIVE SECRETORY PHASE PHASE -Formation of corpus luteum PRE- PHASE -Menstruation -Increase progesterone MENSTRUAL -Decrease estrogen -NO FERTILIZATION; corpus PHASE -Hypothalamus -Decrease luteum degenerates 10 days after -endometrium secretes FSH progesterone -APG (anterior ovulation degenerates pituitary gland) -WITH FERTILIZATION; secretes FSH concepts produces HCG that -Maturation of sustains life corpus luteum; Graafian follicle progesterone level is maintained at -Increased estrogen high level -Hypothalamus stops -Progesterone level decreases FSH & starts LH -Corpus albicans -APG stops FSH & Sloughing off of endometrial starts LH secretion lining MCHN Mark Abejo
- 8. Menstrual Cycle Menstrual Disorders Dysmenorrhea Premenstrual Amenorrhea Menorrhagia Metrorrhagia Syndrome - Primary- -Edema of Primary- -Excessive or - Irregular No known cause lower Never prolonged bleeding in - Secondary- extremities menstruated; bleeding between May be caused by - Abdominal structural/congenit periods tumor/inflammatory bloating al abnormality conditions - Weight gain Secondary– - Headache Cessation of -Breast menstruation tenderness - Depression - Crying - Loss of concentrati on MCHN Mark Abejo