
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (20)
Semelhante a Hyperprolactinema for undergraduate
Semelhante a Hyperprolactinema for undergraduate (20)
Mais de Faculty of Medicine,Zagazig University,EGYPT
Mais de Faculty of Medicine,Zagazig University,EGYPT (12)
Último
Último (20)
Hyperprolactinema for undergraduate
- 3. Prolactin Cell of Origin PRL is 199 polypeptide hormone made by the pituitary lactotrophs.
- 4. Synthesis and metabolism • Normal serum level= 10- 25 ng/ml, • half life =20 minutes • Metabolized in liver and kidney
- 5. Types(isoforms) • Little PRL: • 80-90%, MW 23000K, • non glycosylated • high receptor binding bioactivity • full immuno-activity
- 6. Isoforms • Big PRL: • 8-20%, MW 50000K, mixture of dimeric and trimeric forms of G-PRL • Big-big PRL: • 1-5%, MW 100000K, • polymeric
- 7. Control of prolactin release: • 1- Prolactin inhibiting factor (dopamine) → ↓ prolactin release. • 2- Estrogen → ↑ prolactin release. • 3- TRH “thyrotropin releasing hormone” → ↑ prolactin release.
- 8. – Sleep – Satiety – Stress&Exercise – Sex – Second half Menstrual cycle(luteal phase) – Suckling If a woman's prolactin level is elevated the first time it is tested, a second sample should be checked when she is fasting and non-stressed. Physiologic conditions
- 9. Pharmacological conditions : • -Estrogen containing drugs/ pills. • -Antidopaminergic drugs: • - Tricyclic antidepressant (TCA) • -Anti emetics → meteclopromide. • Antihypertensives: α methyl dopa &reserpine • Histamine H2-receptor antagonists • Stimulation of serotoninergic system Amphetamines Hallucinogens
- 11. Pathological condition • 1. Pituitary: • * Pituitary adenoma "Prolactinoma". • * Growth H. secreting tumor.
- 12. 2. Hypothalamic: • * inhibits PIF (dopamine) secretion or access to pituitary. • * Functional "idiopathic“ *Organic lesion: trauma, infection, tumors. • * Psychological disturbance.
- 13. •A craniopharyngioma is a benign tumor that develops near the pituitary gland . • most commonly in childhood and adolescence and •in later adult life. compresses the pituitary stalk or gland, the tumor can cause partial or complete pituitary hormone de ficiency.
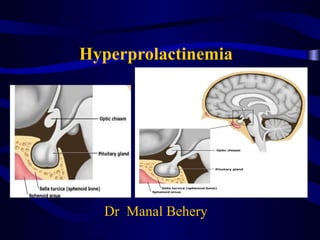
- 14. Diagrammatic representation of empty sella syndrome. A, Normal anatomic relationship. B, C, and D, Progression in development of empty sella syndrome. Note thinning of floor and symmetric enlargement of sella turcica. Empty sella sydrome
- 15. 3. Primary hypothyroidism • ↑ TRH → stimulates lactotrophs to ↑ prolactin secretion.
- 16. Other causes Liver cell failure- Chronic renal failure. Chest wall disease: burn- scar- Herpes Zoster. Ectopic secretion:Hypernephroma of kidney. * Oat cell carcinoma of lung hyperestrogenic states e.g PCO
- 17. Pathologic conditions • Hypothalamic lesions Craniopharyngioma Glioma Granuloma Stalk transection Irradiation damage Pseudocysts • Pituitary tumors Cushing disease Acromegaly Prolactinoma • Reflex causes Chest wall injury herpes zoster neuritis Upper abdominal op • Hypothyroidism • Renal failure • Ectopic pdoduction Bronchogenic carcinoma Hypernephroma
- 20. A- Inhibition of pulsatile GnRH secretion 1- Hyperprolactinemia inhibit GnRH activity by interacting with hypothalamic DA and opioid system via the short-loop feedback mechanism.
- 21. CNS-hypothalamus-pituitary ovary-uterus interaction Neural control Chemical control Dopamine (-) Norepinephrine (+) Endorphins (-) Hypothalamus GnRH Ant. pituitary FS, LHH Ovaries Uterus ProgesteroneEstrogen Menses –± ?
- 22. B. Interference with gonadotrophin action in ovary 2-Decreased ovarian sensitivity to pituitary gonadotropin
- 23. C-Inhibition of FSH-directed ovarian aromatase • 3-impaired follicular development
- 24. D- Inhibition of progesterone synthesis 4-Impaired ovarian strediogensis
- 25. Clinical Manifestation • 1- Galactorrhea: Only in 30- 60 % of cases of hyperprolactinemia due to : • 2- Infertility: due to:- Anovulation luteal phase defect • 3- Oligohypomenorrhea , even amenorrhea • 4- Hirsutism due to decreased SHBG. • 5 -Decreased libido &osteoporosis
- 26. Diagnosis
- 27. 1- History: • of a cause( Drug intake,thyroid,renal...) • of a symptom (galactorrhea,menstrual problem, ...).
- 28. 2- Examination • - Visual field defect → pituitary adenoma. • - Thyroid → goiter. • - Breast → examined for galactorrhea. • - Chest wall → burn, scar.
- 29. 1- Prolactin level: • > 100 ng / ml → suggestive of adenoma. • > 300 ng/ ml → diagnostic of adenoma. • > 2000 ng/ ml→cavernous sinus invasion.
- 30. 2- MRI brain: • - Detect all macroadenoma (> 1cm). • - Detect 70% of microadenoma(<1cm).
- 31. • 3- Thyroid function tests. • 4- Others : - Liver function test. - Kidney function test.
- 32. Treatment of the cause • - Treatment of hypothyroidism (thyroxine). • -stop drugs causing hyperprolactinemia. • -PCO,Liver,renal,.....
- 33. 2- Dopamine agonists: • Acts on D2 receptors but also D1,Alpha adrenergic. • 1. Bromocreptine (parlodel): tablet = 2.5 mg oral or even vaginal.- start with ½ tablet → ↑ gradually ,better during meals. • - Side effects1- Nausea & vomiting. • 2- Postural hypotension.3- Headache. • 4- Abdominal cramps.
- 34. . Lisuride (dopergine): • More potent. - Less side effects.
- 35. 3. Cabergoline (dostinex): • Selective D2 Agonist tablet 0.5 mg • - Long acting. • - More potent. • - Less side effects
- 36. . Quinagolid (norprolac): • non-ergot preparation (D2 receptors), • less side effects
- 37. 3- Trans-sphenoid surgery: • For Pituitary adenoma only if : • - No response to medical ttt. • - Causing visual field defect. • - TTT is not tolerable.