
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Semelhante a Oct 24 CAPHC National Symposium
Semelhante a Oct 24 CAPHC National Symposium (20)
Mais de Glenna Gosewich
Mais de Glenna Gosewich (20)
Último
Último (20)
Oct 24 CAPHC National Symposium
- 5. Child health and inequality Frank Elgar, PhD Associate Professor of Psychiatry Canada Research Chair in Social Inequalities in Child Health Institute for Health and Social Policy McGill University
- 6. What we know The odds that a child is healthy, happy, and doing well in school significantly improve as social class rises This graded social pattern is found in most cultures and areas of health Percentage of children with serious emotional or behavioral difficulties, by age group and family income Source: CDC, 2009 National Health Interview Survey
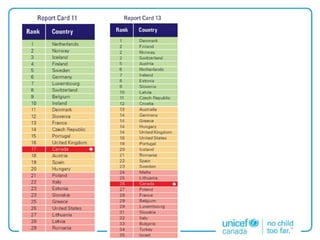
- 7. What we don’t know What happens to child health as we become more unequal? Income inequality and school bullying in 11-year-olds in 37 countries Source: Elgar FJ, Craig W, Morgan A, Vella-Zarb R (2009). Income inequality and school bullying: multilevel study of adolescents in 37 countries. Journal of Adolescent Health, 45(4),351-359.
- 8. Rethinking child poverty Calton, Glasgow Delhi, India
- 9. • National perspectives on health inequality point to the need to improve health services in the most vulnerable groups. • Global perspectives suggest that Canada could do more to tackle the structural determinants of child health that give rise to inequality in the first place. Raise and level the bar Attawapiskat, Ontario
- 10. + “The 42% Problem”: Practical Challenges in the Promotion of Child Wellbeing Charlotte Moore, MD, FRCPC, FAAP Medical Director, Canadian Paediatric Society Assistant Professor, Department of Paediatric Medicine, University of Toronto Staff Paediatrician, Division of Paediatric Medicine, The Hospital for Sick Children
- 11. EVIDENCE POLITICS POLICY OBJECTIVES
- 12. + Total Health Expenditure as % of GDP * Source: OECD Health Data 2012 0 2 4 6 8 10 12 14 16 18 20 1960 1970 1980 1990 2000 2010 United States Canada
- 13. + Total Public Sector Spending Province of Ontario *Source: Ministry of Finance Estimates Operating and Capital Expenses Health Education Social Services Justice Other
- 14. + “Health” / “Illness” Accounting S O C I A L H E A L T H $48B Public Confidence in Health Care System LOS/ Hospitalization for ASC/ Readmission Rates for AMI Rates of Flu Vaccination Median Wait Time for Priority Surgeries Investment in Home Care (Fragile Seniors) Scope of Practice for Allied Health Professions
- 15. + Case Study: Setting Priorities S O C I A L J U S T I C E H E A L T H $109,286 / 28 weeker 1 1. CIHI, Too Early, Too Small: A Profile of Small Babies Across Canada, 2009 2. Cohen, E. et al. Patterns and Costs of Health Care Costs of Children with Medical Complexity, (2012) Pediatrics 130;6. 3. CADTH Canadian Drug Expert Review Committee Final Recommendation – Asfotase Alfa, 2016. H E A L T H H E A L T H 36% 15,771 CMC2 H E A L T H $102 / mg Asfotase Alfa 3
- 16. + Case Study: “Stop FASD” S O C I A L J U S T I C E H E A L T H $3400 / family 1 1. Manitoba Health H E A L T H
- 17. + Case Study: “Stop FASD” E D U C A T I O N S O C I A L J U S T I C E H E A L T H $3400 / family 1 $ 4,596 / year 2 $ 4,075 / year 3 $46,000/year 5 if incarcerated 1. Manitoba Health 2. Stade et al (2009) 3. Stade et al (2009) 5. Fuchs et al (2009) $ 23,760/year 4 if in care 4. Fuchs et al (2008)
Notas do Editor
- I will try to pick the story where Lisa left off, first by framing health inequality from the top to the bottom of the socioeconomic spectrum - not just between the very poor and the rest. and then point to emerging trends on the horizon in rising wealth and inequality, and what these might mean for future population health. Finally I want to touch why we need to rethink what it means to be poor in Canada. First, why focus on economic factors? Many factors contribute to children’s health and wellbeing – stable and supportive family environments, access to health care, access to healthy foods, schools, safe neighbourhoods, access to green spaces and natural environment, and so on. PLUS, health inequalities come in different forms - between gender groups (e.g., rise in anxiety and other mental health problems in adolescent girls), between ethnic and racial groups, between Indigenous and non-Indigenous groups, and between different stages of the life course We could focus on any of these in developing policy that aims to reduce health inequities. I’m sure we would agree that inequality in children’s chances to be healthy are unfair, unnecessary, and costly. But these inequalities all share a similar social pattern, with the most vulnerable groups are nearer to the bottom of the socioeconomic ladder. Income inequality is especially toxic because it exacerbates all the others. It deepens gender inequality, racial inequality, it marginalises immigrant families and reduces their economic mobility. Differences in power, wealth and privilege go a long way to explaining differences in health between these groups. Moreover, - as Lisa has shown us - economic inequality is universal health determinant for all children, including the most advantaged groups.
- Let’s back up a moment... What do we know about socioeconomic differences in child health? There is a graded social pattern in health that is found in most cultures and aspects of health It does not plateau (holds among middle and upper classes) holds after differences in risk factors and access to health services are considered. Is found in both subjective and objective measures of social class; it a psychosocial phenomenon is reinforced by inequalities across many social contexts – children accumulate risk through their exposure to other risk factors, exposure to violence, family dysfunction, the types of peers they have, where they live, the schools they attend Gets “under the skin” at very early age, when the developing brain is most vulnerable to the effects of deprivation.
- None of this is particularly new. What is new here in Canada are soaring economic wealth (GDP) and rising income inequality – ie, gaps between the rich and poor. Income inequality has risen to levels not seen since the 1920s. Wider income differences result in greater social distances across the socioeconomic ladder, so that a child’s socioeconomic position matters more. It reduces the size of the “middle class” and increases levels of relative poverty. {2 clicks to change graphic} Income inequality also contributes to problems that impact everyone’s health - in children and youth we find more mental and physical health problems, more alcohol misuse, more teen pregnancies, more violence (physical assaults and school bullying) More unequal societies have worse health outcomes, particularly in areas where chronic stress plays a role: obesity, diabetes, and mental illness. In our research, we have also found – as you’ve intuited by now - that socioeconomic differences in adolescent health have increased in tandem with these trends in income inequality – in BMIs, sedentary behaviour, and mental and physical health symptoms. It is a depressing, self-reinforcing cycle: Income inequality reduces social mobility and increases inequality in child well-being. Around the world, it’s the more egalitarian societies – not necessarily the richest – that have better child health outcomes, and are topping UNICEF’s RCs. Canada sits at the back of the pack.
- The ‘sequela’ of wealth and inequality mean that we need to rethink what it means to be poor in a rich country like Canada A child can grow up poor in the absolute sense of the word, like lacking access to nutritious food, having a safe home environment, or having access to health care. There are children in Canada who live in absolute poverty, but it is rare. However a child can also be poor in a relative sense, in that he or she does not meet an acceptable standard of living that is set by the rest of society. Income inequality is really about relative poverty. or “relative deprivation” and it is determined by 2 things: your status or rank in society and the amount of inequality around you. And despite an astonishing level of material wealth and technological achievement here in Canada, relative poverty remains a powerful determinant of child well-being. I would argue that it will be come even more powerful in the future. I’ll borrow an example from Michal Marmot (of UCL, of the WHO Commission on the SDH, Whitehall studies)… In the poorest area of Glasgow, Scotland, the life expectancy for males is 54. In India, three-quarters of the population lives on just $2 per day or less. No one in Glasgow is living on $2 per day, and yet their life expectancy is 8 years shorter. Relative disadvantage and the gradient effect on health are what shapes and constrains the wellbeing of Canada’s youth.
- I find it difficult to conceive how Canada will improve is international rankings in child well-being without reducing health inequality in this country, which – as I hope we can agree – is linked to the distribution of wealth. You may remember the late Clyde Hertzman, who spoke at this conference, said that the social gradient ‘flattens up.’ If you want to improve the average then you need to level the bar. Health interventions often have the greatest effects in the most advantaged group in society. This might improve the average a bit while creating even wider inequalities So the last point I want to make speaks to how we can frame the problem of inequality in ways that leads us to a better policy It seems that local and national perspectives on health inequalities focus on vulnerable groups and whether our gov’t is doing enough. For example, it is time now that our current Federal Government, which during the election ran on promises to increase funding to Indigenous communities to bring their health and social services up to the national average, to start coming through with results. Bringing these services up to par is the least we should expect; if achieving health equity is the goal then we really need a disproportionate response, and considerably more support than the average. We might easily feel frustrated with our government for a lack of progress on this file, without thinking about impacts of our comfy lifestyles in widening the social divide, while loosing sight of the larger, ‘more upstream’ social determinant. I have found that in global health research, the data point more directly to those structural determinants. A problem like income inequality in Canada is more apparent when we compare Canada to similarly rich countries. We spend much more on accommodating the health impacts of inequality and do very little to prevent inequality in the first place. Let me leave it with this thought: Robert Sapolsky, an endocrinologist at Stanford University, once noted, “the surest way to feel poor is to be endlessly made aware of the haves when you are a have-not” Most of us in this room enjoys a reasonably comfortable standard of living. It may seems less adequate when we ‘look up’ at the abundance of wealth held by a few at the top. But no one looks down, or thinks – for the millions of children living in relative poverty - about their VIEW FROM THE BOTTOM.
- Thank you so much for inviting me to speak here today – I hope that I am able to share with you some very practical challenges that face us all who are committed to the challenge of disease prevention and the promotion of wellbeing in children, And also to share with you some ideas for re-framing the dialogue for the future – a frame that may offer to us some potential solutions.
- GLARING disconnect between our evidence base, our political rhetoric and our public policy choices. Investing in children – investing in citizens early in their life course – should be an obvious “best choice” for public funds. We know from the work of Neal Halfon, from Paul Wise, from Jean Clinton, from Robin Williams, from Clyde Hertzman, (and so many others – from basic scientists to social scientists – represented here in Figure 1) that there IS a unique and time-limited opportunity to significantly alter one’s lifetime health, wellbeing and productivity by investing in citizens as children. Investing in children aligns with our public expectations, our community ethics, and provides an otherwise exceedingly attractive political narrative. And investing in children provides, over an extended time horizon, a valuable return on investment. This is one of those precious and rare instances where the evidence apparently aligns with politics aligns with policy objectives. It should be a no brainer. So why is it so very hard? Why is child health such a difficult “sell”? Why do our issues capitvate such a small proportion of the public and political dialogue, and why are our issues so rarely at the center of the political agenda?
- The epidemiologic, demographic and technological realities of modern medicine provide near limitless capacity to justify further investment in the health sector. Over the last sixty years – and intensified in the last ten -- the justification has worked. We are spending lots and lots of money – ever more, in fact -- on health. We are all familiar with the dramatic curves that demonstrate Total Health Expenditure per capita. Made even more dramatic when you consider that GDP growth has been nearly flay So, combined, what we have is a staggering and fully unsustainable growth in total health expenditure as a PERCENTAGE of GDP. This is where the challenge lies.
- What is the 42% problem? In Ontario, as in jurisdictions across both Canada and the United States, Health care (here represented in purple) has grown to 42% of all public spending.
- ACS-conditions, Readmission Rates, Flu vaccination – Decease demand for $48 Billion Wait Times, 5-Year Survival, HALE – Increase trust in public health system, warrenting future investments in health This all makes sense. Rational. Logically. Carefully planned and executed. AND the very reason why theWellbeing-Oriented Life Course Health Policy approach is such a impossible sell.
- CMC experiencing a hospitalization over a 2-year period constitute approximately two-thirds of a percent of the population of children in Ontario but account for almost one-third of health care spending on all children. Asfotase alfa a specific enzyme replacement therapy product for the treatment of pediatric hypophosphatasiais priced at $102/mg. At the recommended dose of 2 mg/kg of body weight three times per week or 1 mg/kg of body weight six times per week, the annual cost will exceed $1 million for patients weighing more than 20 kg.
- It is not a priority because we organize our public sector budgets, and funding by sectors…. If the problem is defined as the “42% problem” – We will never effectively and efficiently address the complex, life-course-oriented child wellbeing issues that matter to us – like FASD. Because that would require “bending the curve” in the “wrong” direction – Investing MORE in healthcare. Turning the 42% problem into a 43, or 44, or 45% problem….. And this further investment in health….will not “return” to health. It cannot be measured by health. And, therefore, it will not be “spent” by health.
- It is not a priority because we organize our public sector budgets, and funding by sectors…. If the problem is defined as the “42% problem” – We will never effectively and efficiently address the complex, life-course-oriented child wellbeing issues that matter to us – like FASD. Because that would require “bending the curve” in the “wrong” direction – Investing MORE in healthcare. Turning the 42% problem into a 43, or 44, or 45% problem….. And this further investment in health….will not “return” to health. It cannot be measured by health. And, therefore, it will not be “spent” by health.