

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (17)
Semelhante a poster FF
Semelhante a poster FF (20)
poster FF
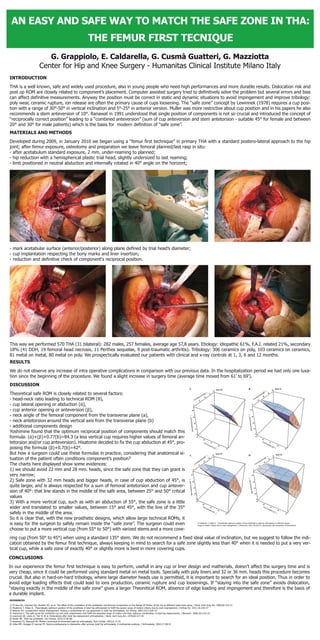
- 1. CONCLUSIONS In our experience the femur first technique is easy to perform, usefull in any cup or liner design and matherials, doesn’t affect the surgery time and is very cheap, since it could be performed using standard metal on metal tools. Specially with poly liners and 32 or 36 mm. heads this procedure becomes crucial. But also in hard-on-hard tribology, where large diameter heads use is permitted, it is important to search for an ideal position. Thus in order to avoid edge loading effects that could lead to ions production, ceramic rupture and cup loosenings. If “staying into the safe zone” avoids dislocation, “staying exactly in the middle of the safe zone” gives a larger Theoretical ROM, absence of edge loading and impingement and therefore is the basis of a durable implant. DISCUSSION Theoretical safe ROM is closely related to several factors: - head-neck ratio leading to technical ROM (θ), - cup lateral opening or abduction (ά), - cup anterior opening or anteversion (β), - neck angle of the femoral component from the transverse plane (a), - neck antetorsion around the vertical axis from the transverse plane (b) - additional components design Yoshimine found that the optimum reciprocal position of components should match this formula: (ά)+(β)+0.77(b)=84.3 (a less vertical cup requires higher values of femoral an- tetorsion and/or cup anteversion). Hisatome decided to fix the cup abduction at 45°, pro- posing the formula (β)+0.7(b)=42°. But how a surgeon could use these formulas in practice, considering that anatomical si- tuation of the patient often conditions component’s position? The charts here displayed show some evidences: 1) we should avoid 22 mm and 28 mm. heads, since the safe zone that they can grant is very narrow; 2) Safe zone with 32 mm heads and bigger heads, in case of cup abduction of 45°, is quite larger, and is always respected for a sum of femoral antetorsion and cup antever- sion of 40°: that line stands in the middle of the safe area, between 25° and 50° critical values 3) With a more vertical cup, such as with an abduction of 55°, the safe zone is a little wider and translated to smaller values, between 15° and 45°, with the line of the 35° safely in the middle of the area. So it is clear that, with the new prosthetic designs, which allow large technical ROMs, it is easy for the surgeon to safely remain inside the “safe zone”. The surgeon could even choose to put a more vertical cup (from 55° to 50°) with varized stems and a more cove- ring cup (from 50° to 45°) when using a standard 135° stem. We do not recommend a fixed ideal value of inclination, but we suggest to follow the indi- cation obtained by the femur first technique, always keeping in mind to search for a safe zone slightly less than 40° when it is needed to put a very ver- tical cup, while a safe zone of exactly 40° or slightly more is best in more covering cups. © Hisatome T, Hideo D. Theoretically optimum position of the prosthesis in total hip arthroplasty to fulfill the severe range of motion criteria due to neck impingement, J Orthop Sci. 2011;16:229-37, reproduced with permission of the Authors RESULTS We do not observe any increase of intra operative complications in comparison with our previous data. In the hospitalization period we had only one luxa- tion since the beginning of the procedure. We found a slight increase in surgery time (average time moved from 61’ to 69’). REFERENCES 1) D’Lima DD, Urquhart AG, Buehler KO, et al. The effect of the orientation of the acetabular and femoral components on the Range Of Motion of the hip at different head-neck ratios, J Bone Joint Surg Am. 2000;82:315-21 2) Hisatome T, Hideo D. Theoretically optimum position of the prosthesis in total hip arthroplasty to fulfill the severe range of motion criteria due to neck impingement, J Orthop Sci. 2011;16:229-37 3) Widmer KH. Containment versus impingement: finding a compromise for cup placement in total hip arthroplasty, Int Orthop. 2007;31(1):S29-33 4) Yoshimine F. The safe-zones for combined cup and neck anteversions that fulfill the essential range of motion and their optimum combination in total hip replacements, J Biomech. 2006;39:1315-23 5) Lewinnek GE, Lewis JL, Tarr R, et al. Dislocations after total hip-replacement arthroplasties, J Bone Joint Surg Am. 1978;60:217-20 6) Muller ME. Total hip prosthesis. Clin Orthop. 1970;72:46-68 7) Ranawat CS, Maynard MJ. Modern technique of cemented total hip arthroplasty, Tech Orthop. 1991;6:17-25 8) Jolles BM, Zangger P, Leyvraz PF. Factors predisposing to dislocation after primary total hip arthroplasty. A multivariate analysis, J Arthroplasty. 2002;17:282-8 This way we performed 570 THA (31 bilateral): 282 males, 257 females, average age 57,8 years. Etiology: idiopathic 61%, F.A.I. related 21%, secondary 18% (41 DDH, 19 femoral head necrosis, 11 Perthes sequelae, 9 post-traumatic arthritis). Tribology: 306 ceramics on poly, 103 ceramics on ceramics, 81 metal on metal, 80 metal on poly. We prospectically evaluated our patients with clinical and x-ray controls at 1, 3, 6 and 12 months. - mark acetabular surface (anterior/posterior) along plane defined by trial head’s diameter; - cup implantation respecting the bony marks and liner insertion; - reduction and definitive check of component‘s reciprocal position. MATERIALS AND METHODS Developed during 2009, in January 2010 we began using a “femur first technique” in primary THA with a standard postero-lateral approach to the hip joint; after femur exposure, osteotomy and preparation we leave femoral planned/last rasp in situ: - after acetabulum standard exposure, 2 mm. under-reaming to planned; - hip reduction with a hemispherical plastic trial head, slightly undersized to last reaming; - limb positioned in neutral abduction and internally rotated in 40° angle on the horizont; INTRODUCTION THA is a well known, safe and widely used procedure, also in young people who need high performances and more durable results. Dislocation risk and post op ROM are closely related to component’s placement. Computer assisted surgery tried to definitively solve the problem but several errors and bias can affect definitive measurements. Anyway the position must be correct in static and dynamic situations to avoid impingement and improve tribology: poly wear, ceramic rupture, ion release are often the primary cause of cups loosening. The “safe zone” concept by Lewinnek (1978) requires a cup posi- tion with a range of 30°-50° in vertical inclination and 5°-25° in anterior version. Muller was more restrictive about cup position and in his papers he also recommends a stem anteversion of 10°. Ranawat in 1991 understood that single position of components is not so crucial and introduced the concept of “reciprocally correct position” leading to a “combined anteversion” (sum of cup anteversion and stem antetorsion - suitable 45° for female and between 20° and 30° for male patients) which is the basis for modern definition of “safe zone”.