O CONTROLE NEURAL DA SECREÇÃO BASAL DE GH-HORMÔNIO E SUA IMPORTÂNCIA EM CRIANÇA
•Transferir como DOCX, PDF•
0 gostou•764 visualizações

O documento discute o controle neural da secreção basal do hormônio do crescimento e sua importância em crianças, adolescentes e jovens. A liberação do hormônio do crescimento ocorre de forma irregular e intermitente durante o sono e varia de acordo com a idade, com picos entre 1 a 4 horas após o início do sono profundo. Esses picos durante o sono noturno respondem por 70-80% da secreção diária do hormônio do crescimento.

Recomendados
Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (20)
Destaque
Destaque (16)
Semelhante a O CONTROLE NEURAL DA SECREÇÃO BASAL DE GH-HORMÔNIO E SUA IMPORTÂNCIA EM CRIANÇA
Semelhante a O CONTROLE NEURAL DA SECREÇÃO BASAL DE GH-HORMÔNIO E SUA IMPORTÂNCIA EM CRIANÇA (20)
Mais de Van Der Häägen Brazil
Mais de Van Der Häägen Brazil (20)
Último
Último (9)
O CONTROLE NEURAL DA SECREÇÃO BASAL DE GH-HORMÔNIO E SUA IMPORTÂNCIA EM CRIANÇA
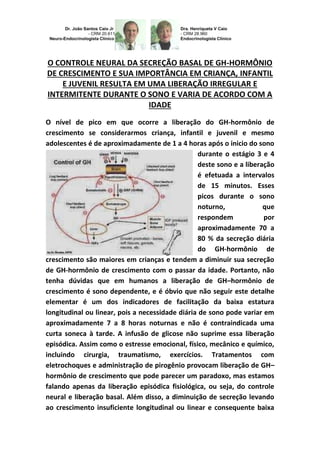
- 1. O CONTROLE NEURAL DA SECREÇÃO BASAL DE GH-HORMÔNIO DE CRESCIMENTO E SUA IMPORTÂNCIA EM CRIANÇA, INFANTIL E JUVENIL RESULTA EM UMA LIBERAÇÃO IRREGULAR E INTERMITENTE DURANTE O SONO E VARIA DE ACORDO COM A IDADE O nível de pico em que ocorre a liberação do GH-hormônio de crescimento se considerarmos criança, infantil e juvenil e mesmo adolescentes é de aproximadamente de 1 a 4 horas após o inicio do sono durante o estágio 3 e 4 deste sono e a liberação é efetuada a intervalos de 15 minutos. Esses picos durante o sono noturno, que respondem por aproximadamente 70 a 80 % da secreção diária do GH-hormônio de crescimento são maiores em crianças e tendem a diminuir sua secreção de GH-hormônio de crescimento com o passar da idade. Portanto, não tenha dúvidas que em humanos a liberação de GH–hormônio de crescimento é sono dependente, e é óbvio que não seguir este detalhe elementar é um dos indicadores de facilitação da baixa estatura longitudinal ou linear, pois a necessidade diária de sono pode variar em aproximadamente 7 a 8 horas noturnas e não é contraindicada uma curta soneca à tarde. A infusão de glicose não suprime essa liberação episódica. Assim como o estresse emocional, físico, mecânico e químico, incluindo cirurgia, traumatismo, exercícios. Tratamentos com eletrochoques e administração de pirogênio provocam liberação de GH– hormônio de crescimento que pode parecer um paradoxo, mas estamos falando apenas da liberação episódica fisiológica, ou seja, do controle neural e liberação basal. Além disso, a diminuição de secreção levando ao crescimento insuficiente longitudinal ou linear e consequente baixa
- 2. estatura (altura) foi bem documentada em criança, infantil e juvenil com grave privação emocional. Entretanto, o descontrole metabólico é um forte comprometedor do GH-hormônio de crescimento e metabolismo: os fatores metabólicos que afetam a secreção de GH incluem todos os substratos energéticos; carboidratos, proteínas e gordura. A administração de glicose por via oral ou intravenosa diminui a liberação de GH em indivíduos sadios. A hipoglicemia, por sua vez, estimula a liberação de GH-hormônio de crescimento. Esse efeito depende de glicopenia intracelular, pois a administração de 2-desoxiglicose (um análogo da glicose que leva à deficiência intracelular de glicose) também aumenta o GH. Essa resposta à hipoglicemia depende da taxa de variação da glicose no sangue e do nível absoluto atingido. O que podemos deduzir do controle neural é que: o sistema hipotálamo-hipofisário compõe o sistema de regulação neuroendócrina. As conexões entre o sistema nervoso e o sistema endócrino, dentre outras vias, ocorre principalmente pelo eixo hipotálamo-hipofisário. O controle neural ocorre através de neurotransmissores, já a regulação endócrina ocorre por hormônios ou neurohormônios. Os hormônios adeno-hipofisários respondem a fatores de estimulação/inibição hipotalâmicos. Os hormônios da neurohipófise são sintetizados pelos próprios neurônios que chegam a neurohipófise. O controle da secreção dos hormônios hipotalâmicos-hipofisários é regulado por alças de feedback: longas (onde os órgãos endócrinos respondem com secreção hormonal contra- regulando a secreção central), curtas (a hipófise contra-regula o hipotálamo) e ultracurtas (onde o hipotálamo contra-regula o próprio hipotálamo).
- 3. THE NEURAL CONTROL, BASAL SECRETION OF GH-GROWTH HORMONE AND ITS IMPORTANCE TO CHILD, INFANT AND YOUTH. THE NEURAL CONTROL OF GH SECRETION BASEMENT-GROWTH HORMONE AND ITS IMPORTANCE IN CHILD, INFANT AND YOUTH RESULTS IN AN ILLEGAL RELEASE AND FLASHING DURING SLEEP AND VARY ACCORDING TO AGE: PHYSIOLOGY-ENDOCRINOLOGY- NEUROENDOCRINOLOGY-GENETICS-ENDOCRINE-PEDIATRICS (SUBDIVISION OF ENDOCRINOLOGY): DR. JOÃO SANTOS CAIO JR. ET DRA. HENRIQUETA VERLANGIERI CAIO. The peak level in which GH-Growth Hormone release occurs considering child, infant and young people and even teenagers is approximately 1 to 4 hours after the onset of sleep during stage 3 and 4 of sleep and the release is performed at intervals of approximately 15 to 15 minutes. These peaks during nighttime sleep, which account for approximately 70 a 80% of daily GH secretion higher growth hormone are in children and tend to decrease their secretion of with increasing age. Therefore have no doubt that humans are dependent on sleep when it comes to release of GH, and of course that does not follow this basic detail is one of the indicators to facilitate low because the need daily longitudinal or linear height of Sleep can vary by about 7 to 8 hours nightly and is not contraindicated in the afternoon a short nap. The glucose infusion does not suppress this episodic release. The same occurs with emotional stress, physical,
- 4. mechanical and chemical, including surgery, trauma and exercise. Electroshock treatments and administration of pyrogen causes the release of GH which may seem a paradox, but we are only talking about the physiological episodic release, e.g., the neural control and basal release. Moreover, the decrease in secretion leading to longitudinal or linear and consequent short stature (height) insufficient growth has been well documented in child, infant and youth with severe emotional deprivation. However, the metabolic disorder is a strong binding of GH and Metabolism: metabolic factors affecting GH secretion include all energy substrates, carbohydrates, proteins and fat. The administration of glucose by oral or intravenous decreases GH in healthy individuals. The hypoglycemia, in turn, stimulates release of GH. This effect depends on intracellular glicopenia, because the administration of 2-deoxyglucose (an analogue of glucose that leads to intracellular glucose deficiency) also increases GH. This response to hypoglycemia depends on the rate of change in blood glucose level and the absolute achieved. What we can deduce is that the neural control? The hypothalamus-pituitary system composes the system neuroendocrine regulation. The connections between the nervous system and the endocrine system, among other routes, occur primarily by the hypothalamus-pituitary axis. The neural control occurs via neurotransmitters, since endocrine regulation occurs through hormones or neurohormones. The adeno pituitary hormones respond to stimulation/inhibition of hypothalamic factors. Neurohypophysis hormones are synthesized by the neurons that reach the neurohypophysis.
- 5. Control the secretion of pituitary hormones is regulated by hypothalamic feedback loops: long (where the endocrine organs respond to hormone secretion from the central regulating secretion), short (against the pituitary regulates the hypothalamus) and ultra short (where the hypothalamus regulates against hypothalamus itself). Dr. João Santos Caio Jr. Endocrinologia – Neuroendocrinologista CRM 20611 Dra. Henriqueta V. Caio Endocrinolgista – Medicina Interna CRM 2893 Como saber mais: 1. Cerca de 1 em 3.500 crianças nos EUA são diagnosticadas com DGH (Lindsay et al. 1994). Apenas 20% destas crianças têm DGH orgânica... http://hormoniocrescimentoadultos.blogspot.com 2. As causas orgânicas incluem tumores do sistema nervoso central, radiação, infecção e lesão cerebral traumática... http://longevidadefutura.blogspot.com 3. Aproximadamente 80% das crianças não têm uma causa prontamente identificável de DGH. Estes pacientes são classificados como tendo DGH idiopática... http://imcobesidade.blogspot.com AUTORIZADO O USO DOS DIREITOS AUTORAIS COM CITAÇÃO DOS AUTORES PROSPECTIVOS ET REFERÊNCIA BIBLIOGRÁFICA. Referências Bibliográficas: Caio Jr, João Santos, Dr.; Endocrinologista, Neuroendocrinologista, Caio,H. V., Dra. Endocrinologista, Medicina Interna – Van Der Häägen Brazil, São Paulo, Brasil; ABE H., CHIHARA K., CHIBA T.,
- 6. MATSUKURA S., FUJITA T. (1981) Effect of intraventricular injection of neurotensin and various bioactive peptides on plasma immunoreactive somatostatin levels in rat hypophysial portal blood. Endocrinology 108:1939–1943; ABE H., KATO Y., IWASAKI I., CHIHARA K., IMURA H.(1978) Central effect of somatostatin on the secretion of growth hormone in the anesthetized rat. Proc. Soc. Exp. Biol. Med. 159:346–349; ABE H., KIMURA K., MINAMITANI N., IWASAKI J. CHIBA T., MATSUKARA S., FUJITA T. (1981) Stimulation by bombesin of immunoreactive somatostatin release into rat hypophysial portal blood. Endocrinology 109:229–234; ABRAMS R. L., GRUMBACH M. M., KAPLAN S. L. (1971) The effect of administration of human growth hormone on plasma growth hormone, cortisol, glucose, and free fatty acid response to insulin: evidence for GH autoregulation in man. J. Clin. Invest. 50:940–950; ABRIBAT T., BOULANGER L., GAUDREAU P. (1990) Characterization of human growth hormone-releasing factor (1–44) amide binding to rat pituitary. Evidence for a high and low affinity classes of sites.Brain Res. 528:291–299; ABRIBAT T., DESLAURIES N., BRAZEAU P., GAUDREAU P. (1991) Alterations of pituitary growth hormone-releasing factor binding sites in aging rats. Endocrinology 128:633–635; ABRIBAT T., FINKELSTEIN J. A., GAUDREAU P. (1991) Alterations of somatostatin but not growth hormone-releasing factor pituitary binding sites in obese Zucker rats. Regul. Pept. 36:263–270; ACS Z., LONART G., MAKARA G. (1990) Role of hypothalamic factors (growth hormone-releasing hormone and gamma-aminobutyric acid) in the regulation of growth hormone secretion in the neonatal and adult rat. Neuroendocrinology 52:156–160; ACS Z., MAKARA G. B., STARK E.(1984) Growth hormone secretion of the neonatal rat pituitaries is stimulated by gamma- aminobutyric acid in vitro. Life Sci. 34:1505–1511; ACS Z., SZABO B., KAPOCS G., MAKARA G. B. (1987) γ-Aminobutyric acid stimulates pituitary growth hormone secretion in the neonatal rat. A superfusion study. Endocrinology 120: 1790–1798; ACS Z., ZSOM L., MAKARA G. B.(1992) Possible mediation of GABA induced growth hormone secretion by increased calcium-flux in neonatal pituitaries. Life Sci. 50:217–279. Contato: Fones: 55 11 5087-4404 ou 96197-0305 Nextel: ID:111*101625 Rua Estela, 515 - Bloco D - 12º andar - Conj. 121/122 Paraiso - São Paulo - SP - Cep 04011-002 e-mails: drcaio@vanderhaagenbrasil.com drahenriqueta@vanderhaagenbrasil.com vanderhaagen@vanderhaagenbrasil.com Site Van Der Häägen Brazil www.vanderhaagenbrazil.com.br www.clinicavanderhaagen.com.br www.crescimentoinfoco.com www.obesidadeinfoco.com.br http://drcaiojr.site.med.br http://dracaio.site.med.br
- 7. Joao Santos Caio Jr http://google.com/+JoaoSantosCaioJr Video http://youtu.be/woonaiFJQwY Google Maps: http://maps.google.com.br/maps/place?cid=5099901339000351730&q=Van+Der+Haagen+Brasil&hl= pt&sll=-23.578256,46.645653&sspn=0.005074,0.009645&ie =UTF8&ll=-23.575591,- 46.650481&spn=0,0&t = h&z=17