Recommended

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Cardiovascular and diabetes risk profiles of children and adolescents attending diabetes screening clinics in rural Alberta according to ethnicity
Similar to Cardiovascular and diabetes risk profiles of children and adolescents attending diabetes screening clinics in rural Alberta according to ethnicity (20)
More from Kelli Buckreus
More from Kelli Buckreus (14)
Cardiovascular and diabetes risk profiles of children and adolescents attending diabetes screening clinics in rural Alberta according to ethnicity
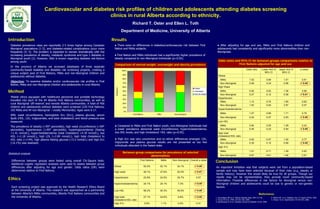
- 1. Cardiovascular and diabetes risk profiles of children and adolescents attending diabetes screening clinics in rural Alberta according to ethnicity. Richard T. Oster and Ellen L. Toth Department of Medicine, University of Alberta Introduction Diabetes prevalence rates are reportedly 2-5 times higher among Canadian Aboriginal populations (1-3), and diabetes-related complications occur more frequently (4, 5). The problem is expected to worsen dramatically with the increasing prevalence of obesity, metabolic syndrome and type 2 diabetes in Aboriginal youth (2). However, little is known regarding diabetes risk-factors among youth. In the province of Alberta we accessed databases of three separate community-based diabetes and diabetes risk screening projects, creating a unique subject pool of First Nations, Métis and non-Aboriginal children and adolescents without diabetes. Objective: To examine diabetes and/or cardiovascular risk profiles in First Nation, Métis and non-Aboriginal children and adolescents in rural Alberta. Method Mobile clinics equipped with healthcare personnel and portable technology travelled into each of the 44 Alberta First Nations communities, as well as rural Aboriginal ‘off-reserve’ and remote Alberta communities. A total of 456 children and adolescents without diabetes were screened (220 First Nations, 192 Métis and 44 non-Aboriginal – mostly Mennonite). Ages were 6-17. BMI, waist circumference, hemoglobin A1c (A1c), plasma glucose, serum lipids (HDL, LDL, triglycerides, and total cholesterol) and blood pressure was measured. The prevalence of obesity (>95th percentile), high waist circumference (>90th percentile), hypertension (>95th percentile), hypertriglyceridemia (fasting >1.41 mmol/L), hypercholesterolemia (total cholesterol >4.39 mmol/L), low HDL (<1.18 mmol/L), high LDL (>2.84 mmol/L), high total cholesterol to HDL ratio (>3.94), high plasma fasting glucose (>5.5 mmol/L) and high A1c (>6.1%) was assessed. Conclusion Between group comparisons for prevalence of selected abnormalities Differences between groups were tested using overall Chi-Square tests. Additional Logistic regression analyses were used to assess between group differences after adjusting for age and gender. Odds ratios (OR) were determined relative to First Nations. Each screening project was approved by the Health Research Ethics Board at the University of Alberta. This research was approached as a partnership between Alberta’s Métis communities, Alberta First Nations communities and the University of Alberta. References 1. Hemmelgarn BR et al. Alberta Diabetes Atlas. 2007:127-40. 4. Molitch ME et al. Diabetes Care. 27 Suppl1:S79-83, 2004. 2. Young TK et al. CMAJ. 163:561-566, 2000. 5. Zhang Y et al. Hypertension. 47:410-414, 2006. 3. Dannenbaum D et al. Canadian Journal of Diabetes. 32:46, 2008. Statistical analysis Ethics Results First Nations Métis Non-Aboriginal Overall p-value Obese 50.5% 52.1% 34.1% < 0.05 High waist 49.1% 47.6% 20.5% < 0.01 Hypertension 23.6% 24.5% 35.7% 0.07 Hypercholesterolemia 24.1% 25.1% 7.3% < 0.05 Low HDL 56.2% 50.3% 36.6% < 0.05 High total cholesterol:HDL ratio 27.1% 24.6% 9.8% < 0.05 High A1c 0.9% 1.1% 0.0% 0.31 Odds ratio Lower limit of 95% CI Upper limit of 95% CI p-value Obese Métis 1.02 0.69 1.51 0.91 Non-Aboriginal 0.48 0.24 0.96 < 0.05 High Waist Métis 0.92 0.62 1.36 0.68 Non-Aboriginal 0.27 0.12 0.58 < 0.01 Hypertension Métis 1.12 0.70 1.80 0.63 Non-Aboriginal 1.93 0.94 3.97 0.07 Hypercholesterolemia Métis 1.07 0.66 1.71 0.79 Non-Aboriginal 0.24 0.07 0.83 < 0.05 Low HDL Métis 0.84 0.55 1.29 0.43 Non-Aboriginal 0.46 0.23 0.94 < 0.05 High total cholesterol:HDL ratio Métis 0.93 0.57 1.52 0.77 Non-Aboriginal 0.30 0.10 0.89 < 0.05 High A1c Métis 1.01 0.71 1.49 0.93 Non-Aboriginal 0.97 0.61 1.48 0.91 Comparison of normal weight, overweight and obesity prevalence ● There were no differences in diabetes/cardiovascular risk between First Nation and Métis subjects. ● First Nation and Métis individuals had a significantly higher prevalence of obesity compared to non-Aboriginal individuals (p<0.05). ● Compared to Métis and First Nation youth, non-Aboriginal individuals had a lower prevalence abnormal waist circumference, hypercholesterolemia, low HDL levels, and high cholesterol: HDL ratio (p<0.05). ● High A1c was very uncommon and no ethnic differences emerged. LDL, triglyceride and plasma glucose results are not presented as too few individuals attended in the fasted state. ● After adjusting for age and sex, Métis and First Nations children and adolescents had consistently and significantly more abnormalities than non- Aboriginals. Odds ratios and 95% CI for between groups comparisons relative to First Nations adjusted for age and sex 0% 10% 20% 30% 40% 50% 60% 70% 80% 90% 100% First Nations Métis Non-Aboriginal Prevalence(%) Obese Overweight Normal weight An important limitation was that subjects were not from a population-based sample and may have been selected because of their risks (e.g. obesity or family history); however this would likely be true for all groups. Though our results may not be representative, they provide novel community-based information. Possible differences in risk factors for Aboriginal versus non- Aboriginal children and adolescents could be due to genetic or non-genetic factors.