British Columbia Medical Journal, December 2010 issue - Smoky air and respiratory health in the 2010 forest fire season, British Columbia
•
1 gostou•294 visualizações

British Columbia Medical Journal, December 2010 issue Please download or visit this entire issue online at http://bcmj.org/issue/december-2010

Recomendados
Mais conteúdo relacionado
Mais de British Columbia Medical Journal
Mais de British Columbia Medical Journal (18)
Último
Último (20)
British Columbia Medical Journal, December 2010 issue - Smoky air and respiratory health in the 2010 forest fire season, British Columbia
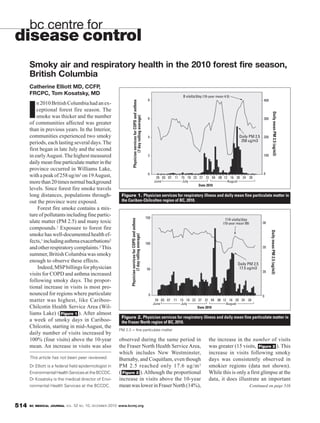
- 1. bc centre for disease control Smoky air and respiratory health in the 2010 forest fire season, British Columbia Catherine Elliott MD, CCFP, FRCPC, Tom Kosatsky, MD 8 visits/day (10-year mean 4.5) 8 400 Physician services for COPD and asthma n 2010 British Columbia had an ex- I ceptional forest fire season. The Daily mean PM 2.5 (ug/m3) smoke was thicker and the number (7 day rolling average) 6 300 of communities affected was greater than in previous years. In the Interior, communities experienced two smoky 4 Daily PM 2.5 200 258 ug/m3 periods, each lasting several days. The first began in late July and the second in early August. The highest measured 2 100 daily mean fine particulate matter in the province occurred in Williams Lake, 0 0 with a peak of 258 ug/m3 on 19 August, 29 03 07 11 15 19 23 27 31 04 08 12 16 20 24 28 more than 20 times normal background June July August Date 2010 levels. Since forest fire smoke travels long distances, populations through- Figure 1. Physician services for respiratory illness and daily mean fine particulate matter in out the province were exposed. the Cariboo-Chilcolten region of BC, 2010. Forest fire smoke contains a mix- ture of pollutants including fine partic- 150 Physician services for COPD and asthma ulate matter (PM 2.5) and many toxic 114 visits/day (10-year mean 99) 30 compounds.1 Exposure to forest fire Daily mean PM 2.5 (ug/m3) smoke has well-documented health ef- (7 day rolling average) fects,1 including asthma exacerbations2 100 and other respiratory complaints.3 This 20 summer, British Columbia was smoky enough to observe these effects. Daily PM 2.5 Indeed, MSP billings for physician 50 17.5 ug/m3 20 visits for COPD and asthma increased following smoky days. The propor- tional increase in visits is most pro- nounced for regions where particulate 0 0 matter was highest, like Cariboo- 29 03 07 11 15 19 23 27 31 04 08 12 16 20 24 28 June July August Chilcotin Health Service Area (Wil- Date 2010 liams Lake) ( Figure 1 ). After almost Figure 2. Physician services for respiratory illness and daily mean fine particulate matter in a week of smoky days in Cariboo- the Fraser North region of BC, 2010. Chilcotin, starting in mid-August, the PM 2.5 = fine particulate matter daily number of visits increased by 100% (four visits) above the 10-year observed during the same period in the increase in the number of visits mean. An increase in visits was also the Fraser North Health Service Area, was greater (15 visits, Figure 2 ). This which includes New Westminster, increase in visits following smoky This article has not been peer reviewed. Burnaby, and Coquitlam, even though days was consistently observed in Dr Elliott is a federal field epidemiologist in PM 2.5 reached only 17.6 ug/m 3 smokier regions (data not shown). Environmental Health Services at the BCCDC. ( Figure 2 ). Although the proportional While this is only a first glimpse at the Dr Kosatsky is the medical director of Envi- increase in visits above the 10-year data, it does illustrate an important ronmental Health Services at the BCCDC. mean was lower in Fraser North (14%), Continued on page 516 514 BC MEDICAL JOURNAL VOL. 52 NO. 10, DECEMBER 2010 www.bcmj.org
- 2. worksafebc Continued from page 515 Evidence Treatment Comments Positive Negative Conflicting Physical therapy Traction or spinal decompression42,43 As a single treatment for any low back pain, with or without sciatica Photonic stimulation44 Interferential stimulation45 Superficial heat or cold46 Short-term with small effect Electromagnetic fields47 For knee osteoarthritis; however, the effect is not clinically significant Electrotherapy48 In treating neck pain For active or passive treatments in whiplash-associated disorders, Conservative therapy49 Grades 1 or 2 Transcutaneous electrical nerve For knee osteoarthritis or chronic low back pain, or in reducing pain stimulation50-54 among patients with rheumatoid arthritis of the hand Low-level laser therapy55,56 In reducing pain among patients with nonspecific low back or neck pain Complementary and alternative medicine Touch therapy, including healing touch, reiki, therapeutic touch57 In reducing pain; however, the effect is not clinically significant Neuroreflexotherapy58 Short-term effect for nonspecific low back pain For nonspecific neck pain Massage 59,60 Small effect for subacute or chronic nonspecific low back pain Evidence, short-term effect in acute headache or chronic Acupuncture61-63 nonspecific low back pain In treating shoulder pain Herbal64,65 For rheumatoid arthritis and maybe low back pain Vitamin D66 References Available on request by e-mailing kukuh.noertjojo@worksafebc.com or calling 604 232-5883. An extended summary of this review is accessible from the Evidence-based Medicine page on WorkSafeBC.com (www.worksafebc.com/evidence.) —Kukuh Noertjojo, MD, MHSc, MSc; Craig Martin, MD, MHSc; Celina Dunn, MD, CCFP WorkSafeBC Evidence-Based Practice Group bccdc Continued from page 514 that patients with chronic respiratory Acknowledgments principle in the relationship between conditions such as COPD and asthma Thank you to Population Health Surveil- air pollution and health: a small in- have rescue medication and emer- lance and Epidemiology, BC Ministry of crease in exposure in large populations gency response plans, and know when Healthy Living and Sport, the Office of the (Fraser North, population 597 659) to seek medical help. Public health res- Provincial Health Officer, and Sarah Hen- can affect larger numbers of people ponses include issuing air quality health derson, environmental health scientist, BC than a large increase in exposures in advisories, establishing air shelters, and Centre for Disease Control. small populations (Cariboo-Chilcotin, evacuating those at risk during severe population 26 646). smoke events. Partnerships between References The evidence we present from this physicians and public health practi- 1. Naeher LP, Brauer M, Lipsett M, et al. season serves as a reminder that forest tioners become particularly advanta- Woodsmoke health effects: A review. fire smoke affects people all over the geous when novel scenarios arise, such Inhal Toxicol 2007;19:67-106. province, even those distant from the as how to manage patients in hospitals 2. Brauer M, Hisham-Hashim M. Fires in fires. Physicians and public health prac- when the indoor air becomes smoky. Indonesia. Environment Science Technol titioners across BC can (and did) work Forest fires are the norm in British 1998;32S:404S-407S. together to reduce the health effects of Columbia, and we can anticipate that 3. Moore D, Copes R, Fisk R, et al. Popula- exposure to forest fires, particularly they will increase with global climate tion health effects of air quality changes among those most at risk: firefight- change. Physicians and public health due to forest fires in British Columbia in ers, young children, the elderly, and practitioners must continue to work 2003: Estimates from physician-visit those with chronic respiratory disease. together to reduce the health impacts billing data. Can J Pub Health 2006; Physicians play a key role in ensuring of forest fires. 97:105-108. 516 BC MEDICAL JOURNAL VOL. 52 NO. 10, DECEMBER 2010 www.bcmj.org