Lyme and syphilis
•Transferir como PPTX, PDF•
4 gostaram•3,945 visualizações

Lyme & Syphilis diseases

Recomendados
Mais conteúdo relacionado
Mais procurados
Mais procurados (17)
Semelhante a Lyme and syphilis
Semelhante a Lyme and syphilis (20)
Mais de Archa Dave
Último
Último (20)
Lyme and syphilis
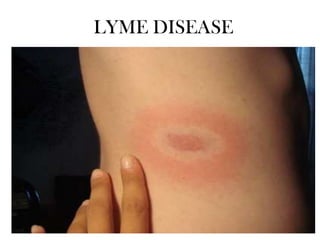
- 1. LYME DISEASE
- 2. • Lyme disease, the most common vector-borne disease, poses a serious health crisis both nationally and internationally. Transmitted by the bite of a tick, Lyme disease is a bacterial infection caused by the spirochete (spiral shaped bacteria) Borrelia burgdorferi. • Lyme disease is a systemic infection that can affect almost any part of the body. Although Lyme disease is the most well known of the tick-borne infections, multiple infections can be transferred at one time by a single tick. • The presence of multiple infections tends to further complicate diagnosis and treatment. • LD occurs endemically in Europe, America and Northern regions of Asia. • In Poland, LD is the most frequent tick borne disease, which causes serious epidemiological problems. • LD is a chronic disease attacking many organs, including the skin, heart, brain and joints.
- 3. • Borrelia burgdorferi is a Gram-negative spirochete bacteria that is well known as the causative agent of Lyme disease. • In 1982, a few years after Lyme disease was first diagnosed, it was determined that B. burgdorferi was being transmitted to humans by ticks. • According to the Centre for Disease Control, Lyme disease caused by B. burgdorferi has become the most common vector-borne bacterial disease in the world. • B. burgdorferi’s unique structure and adaptations allow it to be an effective invasive pathogen and an important organism to research. • Lyme borreliosis is a disease caused by the spirochetes Borrelia burgdorferi, Borrelia afzelii and Borrelia garinii and it is transmitted by ticks. • Most of the proteins (outer surface proteins, flagellar proteins and other uncertain location proteins) have a strong antigenic variability. • Osp A protein genetic and serological studies facilitated the differentiation of seven serotypes strongly correlated with the known genospecies. • The genetic structure of these spirochetes included a large linear chromosome, several linear micro chromosomes as well as a number of circular plasmids. • However, in general, the sequenced genome does not contain any obvious genes coding for pathogenesis, and therefore, the mechanisms of B. burgdorferi infections are still a hot topic of research.
- 5. Ecology • Borrelia burgdorferi is maintained in a natural cycle of infection by ticks. • The ticks acquire and transmit the bacteria by feeding on a variety of small mammals and birds that act as a reservoir host for the Borrelia. • B. burgdorferi is transmitted specifically by ticks of the genus Ixodes, which include a variety of different species found in different geographical locations.
- 6. Pathology • Lyme disease was first identified due to an outbreak of juvenile rheumatoid arthritis. • This is one of the later stage symptoms of the B. burgdorferi infection. • Ticks use many small mammals to harbour the bacteria, and humans only become inadvertently infected when bitten. It is believed that the bacteria use a variety of mechanisms to evade the host immune response. • This includes up regulating certain outer surface proteins, or attaching themselves to immunosuppressive tick salivary proteins. • Once the Borrelia has entered the host, it becomes very invasive and can spread quickly throughout the entire system.
- 7. Continued: • The first sign of infection is the erythema migrans, a circular rash at the site of the tick bite that appears after a few days delay. • From there, infected humans may develop similar rashes on other sites of the body as well as symptoms such as fatigue, fever, headache, and muscle and joint aches. • If the infection spreads throughout the body it has reached Stage II of the infection, which is marked by symptoms such as facial palsy, meningitis, extreme joint pain and heart palpitations. • If it is left untreated for a few months the infection will reach Stage III and patients may develop arthritis as well as severe joint pain and swelling.
- 8. Lyme disease transmission • The Lyme disease bacterium, Borrelia burgdorferi, is spread through the bite of infected ticks. • The blacklegged tick (or deer tick, Ixodes scapularis) spreads the disease in the north-eastern, mid-Atlantic, and north-central United States, and the western blacklegged tick (Ixodes pacificus) spreads the disease on the Pacific Coast. • Ticks can attach to any part of the human body but are often found in hardto-see areas such as the groin, armpits, and scalp. In most cases, the tick must be attached for 36-48 hours or more before the Lyme disease bacterium can be transmitted. • Most humans are infected through the bites of immature ticks called nymphs. Nymphs are tiny (less than 2 mm) and difficult to see; they feed during the spring and summer months. • Adult ticks can also transmit Lyme disease bacteria, but they are much larger and may be more likely to be discovered and removed before they have had time to transmit the bacteria. • Adult Ixodes ticks are most active during the cooler months of the year.
- 9. Laboratory testing • Test for Lyme disease measures antibodies made by white blood cells in response to infection. It can take several weeks after infection for the body to produce sufficient antibodies to be detected. • Therefore, patients tested during the first few weeks of illness will often test negative. • In contrast, patients who have had Lyme disease for longer than 4-6 weeks, especially those with later stages of illness involving the brain or the joints, will almost always test positive. • A patient who has been ill for months or years and has a negative test almost certainly does not have Lyme disease as the cause of their symptoms.
- 10. • Several laboratories offer "in-house" testing for Lyme disease using their own assays or testing criteria. • Such in-house assays do not require evaluation or approval by the Food and Drug Administration (FDA). • Because of the potential for misleading results, CDC and FDA recommend against using in-house assays whose accuracy and clinical usefulness have not been adequately validated. Unvalidated tests available as of 2011 include: • Capture assays for antigens in urine • Culture, immunofluorescence staining, or cell sorting of cell wall-deficient or cystic forms of B. burgdorferi • Lymphocyte transformation tests • Quantitative CD57 lymphocyte assays • “Reverse Western blots” • In-house criteria for interpretation of immunoblots • Measurements of antibodies in joint fluid (synovial fluid) • IgM or IgG tests without a previous ELISA/EIA/IFA
- 11. Treatment • Patients treated with appropriate antibiotics in the early stages of Lyme disease usually recover rapidly and completely. • Antibiotics commonly used for oral treatment include doxycycline, amoxicillin, or cefuroxime axetil. • Patients with certain neurological or cardiac forms of illness may require intravenous treatment with drugs such as ceftriaxone or penicillin. • Approximately 10-20% of patients (particularly those who were diagnosed later), following appropriate antibiotic treatment, may have persistent or recurrent symptoms and are considered to have Post-treatment Lyme disease syndrome (PTLDS). • The National Institutes of Health (NIH) has funded several studies on the treatment of Lyme disease which show that most patients recover when treated with a few weeks of antibiotics taken orally.
- 12. Syphilis
- 13. Syphilis • Syphilis is a highly contagious disease spread primarily by sexual activity, including oral and anal sex. • Occasionally, the disease can be passed to another person through prolonged kissing or close bodily contact. • Although this disease is spread from sores, the vast majority of those sores go unrecognized. • The infected person is often unaware of the disease and unknowingly passes it on to his or her sexual partner. Description: • Treponema pallidum is a Gram-negative bacteria which is spiral in shape. • It is an obligate internal parasite which causes syphilis, a chronic human disease. • Syphilis is a sexually transmitted disease but transmission can also occur between mother and child in utero; this is called congenital syphilis.
- 14. • Syphilis was first discovered in Europe near the end of the fifteenth century. The virulent strain of T. pallidum was first isolated 1912 from a neurosyphilitic patient by Hideyo Noguchi, a Japanese bacteriologist. • Although for the past decades treatment has been available, syphilis remains a health problem throughout the world. • T. pallidum is an important organism because of its ability to cause disease in humans and in efforts to better understand it, its genome was sequenced in July of 1998. • T. pallidum cannot be cultured in the lab and therefore cannot be investigated using conventional lab techniques. • By sequencing its genome, scientists are able to better understand T. pallidum, however many things remain a mystery, most notably what exactly is the virulence factor of this bacteria.
- 15. Cell Structure: • T. pallidum is a Gram-negative bacteria consisting of an inner membrane, a thin peptidoglycan cell wall, and an outer membrane. It is very small in size with a length that ranges from 6 to 20 um and a diameter range of 18-20 um. • T. pallidum is a member of the spirochete family which are characterized by their distinct helical shape. • Probably the most interesting property of T. pallidum’s structure is the endoflagella found in the periplasmic space between its two membranes. • These organelles give T. pallidum its distinctive corkscrew motility. Ecology: • T. pallidum is an obligate internal parasite, meaning that it requires a mammalian host for survival. In the absence of mammalian cells, T. pallidum will be killed by the absence of nutrients, exposure to oxygen and heat. • T. pallidum causes the human disease syphilis. Since T. pallidum cannot be grown in culture, animal models are needed to study syphilis.
- 16. Although mice and monkeys can be used, rabbits are the animal model almost exclusively studied in the lab. Rabbits are used because unlike monkeys they are inexpensive and unlike mice, rabbits develop the signs and symptoms of human primary and secondary syphilis. T. pallidum initially infects the epithelial cells of the genitals during sexual intercourse. From this initial infection site, T. pallidum goes on to infect almost any organ or tissue in the body. A study done using rabbits detected the presence of T. pallidum in the “lymph nodes, brain, and aqueous humor, and in the CSF” after only 18 hours post infection. Another study showed that T. pallidum was then able to travel from the CSF to the eye. T. pallidum has also been found in the blood and liver of infected rabbits.
- 17. Pathology: • • • • • • • T. pallidum is the causative agent of syphilis, a chronic infectious human disease T. pallidum’s virulence factor is still unknown. Untreated, progresses in a series of distinct stages : Primary Secondary Latent tertiary Infection is initiated when T. pallidum penetrates dermal micro abrasions or intact mucous membranes resulting in primary syphilis. Primary syphilis usually presents itself as a single chancre at the site of infection. Secondary syphilis occurs approximately 3 months after infection and presents itself with a variety of symptoms, most notably lesions of the skin and mucous membranes. These include a rash commonly on the palms of the hands, soles of the feet, face, and scalp. The breakdown of mucous membranes appears as patches on lips, inside the mouth, vulva, and vagina. Infected individuals may also experience fever, loss of appetite and weight loss during this stage.
- 18. After several months, secondary symptoms will disappear; this is called the latent phase. Even though the infected individual is no longer showing symptoms, testing confirms that T. pallidum is still present. Transmission at this stage via sexual contact is rare. If untreated, latent phase may progress to tertiary phase. Tertiary syphilis doesn’t manifest until years after initial infection and can affect many different areas of the body. Tertiary syphilis can cause destructive lesions on skin and bones which are usually benign. The more deadly manifestations of late syphilis affect the cardiovascular system (especially the aorta) and the central nervous system causing infected individuals to experience insomnia and changes in personality.
- 19. Laboratory diagnosis Syphilis can be diagnosed by testing samples of: • Blood: Blood tests can confirm the presence of antibodies that the body produces to fight infection. The antibodies to the bacteria that cause syphilis remain in your body for years, so the test can be used to determine a current or past infection. • Fluid from sores: Your doctor may scrape a small sample of cells from a sore to be analysed by microscope in a lab. This test can be done only during primary or secondary syphilis, when sores are present. The scraping can reveal the presence of bacteria that cause syphilis. • Cerebral spinal fluid: If it's suspected that you have nervous system complications of syphilis, your doctor may also suggest collecting a sample of cerebrospinal fluid through a procedure called a lumbar puncture (spinal tap).
- 20. Treatment: • When diagnosed and treated in its early stages, syphilis is easy to cure. • The preferred treatment at all stages is penicillin, an antibiotic medication that can kill the organism that causes syphilis. • A single injection of penicillin can stop the disease from progressing if you've been infected for less than a year. • Penicillin is the only recommended treatment for pregnant women with syphilis. • Women who are allergic to penicillin can undergo a desensitization process that may allow them to take penicillin. • Even if you're treated for syphilis during your pregnancy, your new-born child should also receive antibiotic treatment. • The first day you receive treatment you may experience what's known as the Jarisch-Herxheimer reaction. • Signs and symptoms include fever, chills, nausea, achy pain and headache. This reaction usually doesn't last more than one day.
- 21. Treatment follow-up Have periodic blood tests and exams to make sure you're responding to the usual dosage of penicillin. Avoid sexual contact until the treatment is completed and blood tests indicate the infection has been cured. Notify your sex partners so that they can be tested and get treatment if necessary. Be tested for HIV infection. Prevention: • • • • Abstain or be monogamous. Use a latex condom. Avoid recreational drugs. Screening for pregnant women