Recomendados

Recomendados
Mais conteúdo relacionado
Mais de ABIM Foundation
Mais de ABIM Foundation (9)
Último
Último (20)
Impact of an Interprofessional Central Venous Catheter Insertion Training Program
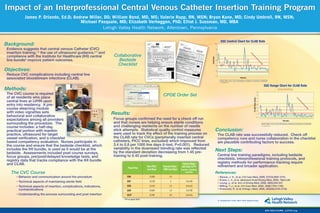
- 1. Impact of an Interprofessional Central Venous Catheter Insertion Training Program James P. Orlando, Ed.D; Andrew Miller, DO; William Bond, MD, MS; Valerie Rupp, RN, MSN; Bryan Kane, MD; Cindy Umbrell, RN, MSN; Michael Pasquale, MD; Elizabeth Verheggen, PhD; Elliot J. Sussman, MD, MBA Lehigh Valley Health Network, Allentown, Pennsylvania SQC Control Chart for CLAB Rate Background: 10 Evidence suggests that central venous Catheter (CVC) 8 insertion training, the use of ultrasound guidance, and 1,2 3,4 compliance with the Institute for Healthcare (IHI) central Collaborative 6 CLAB Rate line bundle improve patient outcomes. 5 Bedside 4 Checklist 2 Objectives: 0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 Reduce CVC complications including central line associated bloodstream infections (CLAB). -2 Months CL CL LCL UCL A Lower bound A Upper bound B Lower bound B Upper bound CL = Control Limit SQC Range Chart for CLAB Rate Methods: (Variability) The CVC course is required CPOE Order Set of all residents who place central lines at LVHN upon entry into residency. A pre- course elearning module with video vignettes sets Results: behavioral and collaborative expectations among all providers Focus groups confirmed the need for a check off run surrounding the procedure. The and that nurses are helping ensure sterile conditions course includes: a half-day and challenging residents on the number of needle practical portion with manikin stick attempts. Statistical quality control measures Conclusion: practice, ultrasound for target were used to track the effect of the training process on The CLAB rate was successfully reduced. Check off vessel verification, and a checklist the CLAB rate for CVCs (peripherally inserted central competency runs and nurse collaboration in the checklist based competency evaluation. Nurses participate in catheters, PICC lines, excluded) which improved from are plausible contributing factors to success. the course and ensure that the bedside checklist, which 3.4 to 0.8 per 1000 line days (t-test, P=0.001). Reduced variability in the downward trending rate was reflected includes the IHI bundle, is used as it would be at the by the standard deviation decreasing from 1.45 pre- Next Steps: bedside. Assessments included post course surveys, focus groups, pre/post/delayed knowledge tests, and training to 0.40 post-training. Central line training paradigms, including bedside registry data that tracks compliance with the IHI bundle checklists, interprofessional training protocols, and and CLAB. Cohorts Begin registry methods for performance tracking require Fiscal Year Non-PICC Infection Rate / with Start of FY refinement and broader application. Line Days 1000 Line Days (Learners = Residents The CVC Course and APCs) References: • Behavior and communication around the procedure 2006 15,004 3.4 1. arsuk, J. H., et al. Crit Care Med, 2009, 37(10):2697-2701. B 2. vans, L. V., et al. (abstract) Acad Emerg Med, 2009, 16(s1):s6. E • echnical aspects of maintaining sterile field T 2007 15,138 2 A (n=56) 3. eung, J., et al. Ann of Emerg Med, 2006, 48(5):540-547. L • echnical aspects of insertion, complications, indications, T 2008 14,136 2.5 B (n=61) 4. illing, T. J., et al. Crit Care Med, 2005, 33(8):1764-1769. M contraindications 5. ronovost, P., et al. N Engl J Med, 2006, 355(26):2725-2732. P 2009 19,463 1.4 C (n=70) • Understanding the process surrounding and post insertion 2010* 15,781 0.8 D (n=61) * FY to April 2010